Richard Malik DVSc PhD FACVS FASM Center for Veterinary Education, University of Sydney
Original article: Treatment of FIP in cats with subcutaneous remdesivir followed by oral GS-441524 tablets
Translator's note: The article contains information about the actual content of GS-441524 in tablets. However, this content may not correspond to the "equivalent" amount of GS-441524 in tablets from other manufacturers, where the actual content of GS-441524 is always slightly higher due to the known reduced bioavailability of the orally used drug. Therefore, it is not possible to simply and unambiguously compare the recommended dosage of GS-441524 from BOVA in Australia and here.
Introduction
Infectious feline peritonitis (FIP) is an infectious disease, especially of young cats. It occurs when a feline enteric coronavirus that multiplies in the gut undergoes a critical mutation that changes its tissue tropism from enterocytes to macrophages. The FIP virus then circulates in the body in macrophages - this is the ultimate mechanism of the Trojan horse. This leads to disseminated infection and the development of fibrinoid necrotizing vasculitis and serositis due to the deposition of immune complexes consisting of feline antibodies and FIP viral antigens.
In general, there are two forms of FIP - effusive ("wet") FIP and non-effusive ("dry") FIP. The disease process itself can occur in the abdomen, thoracic cavity, pericardium, eyes or central nervous system. Combinations of dry and wet FIP with various tissues are not uncommon.
Until recently, the diagnosis of feline infectious peritonitis (FIP) was a death judgment for a feline patient. In recent years, however, this vision has been turned upside down as a result of the pioneering work of Professor Niels C. Pedersen and colleagues at UC Davis.
Over the last 12 months, many veterinarians in Australia have also successfully managed many cases of FIP using remdesivir and GS-441524.
Omega-interferon (Virbagen) and polyprenyl immunostimulant (PPI) were the first drugs used to treat FIP, and both had some effects in some patients. Omega interferon has been useful in cases of effusive ("wet") FIP, often combined with low-dose prednisolone according to the Ishid protocol, while PPI, pioneered by Al Legendre, has been more useful in cases of non-fusible FIP. In some cases, both drugs were used at the same time. The problem was that both forms of therapy were often expensive, especially when both drugs were used, so that although patients improved and could have transient clinical remissions during treatment, permanent clinical cures were rare. As a result, most veterinarians still considered the diagnosis of FIP a prelude to euthanasia.
That all changed a few years ago thanks to the culmination of FIP's lifelong research. Niels Pedersen. Niels is an amazing North American veterinarian of Danish descent. He grew up on a chicken farm and originally wanted to be a clinician for large animals, but with great foresight he decided on a scientific career. Shortly after graduating, he traveled to Canberry to the John Curtin School of Medical Research at ANU, where in the late 1960s he received a PhD in kidney transplant rejection immunology from Professor Bede Morris, using sheep as an experimental model to study lymphocyte kinetics.
When Niels returned to UC Davis, he focused on studying infections and immunity. Although he has contributed to a large number of topics in internal medicine and the genomics of dogs and cats, FIP has become his favorite disease due to its commonness and current complexity. His studies date from the 1980s, when he specialized in diagnostics, virology and pathogenesis, to the present, with an increasing focus on therapy.
Niels, in collaboration with colleagues from Kansas State University, has shown that a purposefully designed protease inhibitor GC-376 could prevent and cure experimentally induced FIP in laboratory cats.1,2 Field clinical trials with cats with naturally occurring disease have been disappointing, especially when cats have had an ocular form of FIP or CNS disease. He did not give up, so he switched to another drug - GS-4415243,4 - a nucleoside analogue developed by the North American pharmaceutical company Gilead. This molecule has been shown to be much more effective than GC-376 in the treatment of FIP, both in experimental infections and in spontaneous cases of FIP. Starting with pharmacokinetics and dose escalation studies using a wide range of clinical cases, Niels and colleagues found that the required dose depended on whether the patient had dry or wet FIP and whether the eye or central nervous system (CNS) was affected.5
Surprisingly, Gilead, the manufacturer who developed GS441524, has not yet shown interest in developing this molecule for the treatment of cats. To fill the gap for effective FIP therapy around the world, various laboratories in China and Eastern Europe have begun producing GS-441524 and selling it on the black market.
The wide availability of the GS-441524, often of high quality and initially very high price, provided dedicated owners with a way to save their cats with FIP. Studies by clinical pathologist Samantha Evans of Ohio State University have indicated a cure rate of approximately 80 % in the field. Until recently, the procurement of the drug was complicated and full of problems, which at some level were circumvented by various "FIP Warriors" groups on Facebook. Unfortunately for Australian cat lovers, APVMA and Vet Boards finally understood what was going on and the Border Force made it much more difficult to obtain GS-441524 and its safe import for veterinary use. Regulatory and Veterinary Committees' warnings against prosecutors were directed against veterinarians who allowed cats with FIP to be treated with black market drugs.
Ironically, the COVID 19 pandemic provided a new solution to this problem. Gilead developed remdesivir (GS-5734) as a drug for the treatment of hepatitis C, Ebola and human coronavirus disease. Remdesivir is a prodrug of GS-441524, which contains an additional chemical side chain (including a phosphate group) to improve intracellular penetration (Figure 1B). Remdesivir (as a product of Veklura) obtained a temporary marketing authorization (for two years) from TGA in July 2020 for the treatment of SARS-CoV-2 infections in human patients with COVID-19. This registration process would normally take several years, but the severity of the pandemic has accelerated this process, taking into account preliminary data from clinical trials. As remdesivir became a licensed human drug and Gilead licensed production worldwide, it meant more access to quality raw material. This circumvented the problems with the use of the drug purchased on the black market, as well as the problems of unknown purity and consistency of the product over time.
In 2020, the veterinary compounding company BOVA Australia provided reliable supplies of remdesivir in a suitable format for IV and subcutaneous application. Studies in Australia have determined that the shelf life after reconstitution exceeds 12 days and have confirmed in vitro efficacy against coronaviruses in tissue cultures. The analytical purity of the drug is regularly checked by HPLC. Over the past year, veterinarians in every Australian state have used remdesivir to treat cats with FIP. There have been a number of effusive and non-fusive cases, including some cats with ocular disorders (uveitis) and others with multifocal CNS disease. Based on treatment of approximately 500 cats treated between October 2020 and November 2021, remdesivir has been shown to be highly effective in managing FIP infections. It allows for a slightly simpler subcutaneous administration and the injection appears to be slightly less painful compared to GS-441524 and does not cause the local injection site reactions observed with GS-441524 injection. Remdesivir was originally used exclusively in Australia, although it has also been available in the UK from BOVA UK for the last 2 months.
The molecular weight of remdesivir is 603 g / mol, while the molecular weight of GS-441524 is 291 g / mol. This could suggest that treatment of cats with remdesivir requires approximately twice the dose of GS-441524, although this does not take into account the possible improvement in intracellular penetration of remdesivir into certain tissues compared to GS-441524. The proposed dose of remdesivir in human patients with COVID19 is 200 mg intravenously (IV), followed by 100 mg IV daily. For a 70 kg human patient, this represents a daily dose of 1.3 mg / kg, so using allometric scaling, a dose of 5-10 mg / kg per day was considered correct for a cat. However, our experience with the first 500 cases was that many cats eventually needed a higher dose of remdesivir for permanent cure, so we adjusted our recommended dosage upwards (see below). Remdesivir provides BOVA as a sterile 10 mg / ml solution ready for use in a 10 ml vial.

At present, Australia and the United Kingdom are the only countries where remdesivir is readily available by prescription for veterinary use. However, veterinarians in India, New Zealand, South Africa and parts of Europe have also started using human medicine suppliers to access the medicine.
Diagnosis

A complete differential diagnosis of FIP is beyond the scope of this article, but readers are strongly encouraged to read the excellent article by Séverine Tasker in the Journal of Feline Medicine & Surgery. 6
Although FIP can occur in cats of any age, most cases occur in kittens and cats less than 3 years of age. Persistent and often high fever that does not respond to antibiotic therapy (and often NSAIDs) is a common finding, as is increased plasma total protein levels due to elevated globulin concentrations (diffuse gammopathy in serum electrophoresis). In effusive or "wet" FIP, the albumin to globulin ratio may drop to <0.45. Acute phase reactants such as serum amyloid A and α1-acid glycoprotein tend to be markedly elevated. Many cats with FIP also exhibit secondary immune-mediated hemolytic anemia, increased AST and ALT activities, and jaundice.
Diagnostic imaging is crucial for early diagnosis, which has been greatly facilitated by the introduction of digital radiology and the widespread availability of diagnostic ultrasound in small animal practice. Pleural effusion is readily recognizable from chest X-rays, while abdominal effusion is best detected by ultrasound (Figure 3), especially if high frequency probes are available. It is worth noting that in some cases, the fluid pockets may be focal and localized. Often there is some fluid around the kidney under the kidney sheath, kittens may have scrotal edema, while in rare cases the discharge is limited to the pericardial sac. But the key is - to look for (i) effusion in any body cavity, (ii) granulomas in the kidneys, liver or lungs, (iii) enlarged intra-abdominal and mesenteric lymph nodes (Figure 5) or marked thickening of the iliac-ecological area (f focal FIP ’) ( Figure 5). Chest X-rays after drainage of pleural effusion may show changes corresponding to viral pneumonia.

If you see an effusion - puncture - because fluid is the best diagnostic sample.

A fluid with a high protein content, often yellow to straw in color, is characteristic (Figure 3B). If you see granuloma in the organ or if the lymph nodes are clearly enlarged - do FNA (thin needle aspiration biopsy), apply a smear, use RapidDiff staining and look for neutrophils and macrophages (pyogranulomatous inflammation) without visible infectious agents (Figure 4). The two diseases most commonly confused with FIP in adult cats are lymphoma and some types of lymphocytic cholangitis (associated with high protein ascites).

Of course, effusive disease is much easier to diagnose because ascitic, pericardial or pleural fluid provides a suitable sample that can be examined cytologically, by fluid analysis and immunofluorescence (IFA) for FIP antigen, or reverse transcriptase PCR to detect FIP nucleic acid. IFA is performed at VPDS, B14, University of Sydney (via Vetnostics, QML, ASAP, VetPath, Gribbles or IDEXX). However, it is usually the cheapest way to send the sample directly to the university laboratory.
Dry FIP is more problematic because it usually requires a thin-needle aspiration biopsy of pyogranulomatous lesions in the liver, kidneys, or abdominal lymph nodes. Occasionally, cases of wet FIP may show fluid samples that are negative for IFA and / or PCR testing, but the patient is still likely to have FIP, which is reflected in a favorable response to remdesivir or GS-441524 treatment.
Treatment
Since October 2020, we have been treating cats with FIP with remdesivir (IV and SCI) and more recently with GS-441524 (oral), so our protocols are constantly evolving with experience. About 500 cats have been treated so far. We try to avoid being too prescriptive in our recommendations, as we suspect that there is no one-size-fits-all protocol and that each case presents unique circumstances, including patient size, whether the cat is still "happy" and reasonably , or is depressed and dehydrated. An important factor is the emotional and financial commitment of the owner. A key feature that needs to be mentioned is that both drugs are very safe, even in sick cats and kittens.
Note that the following recommended doses are higher than those originally recommended a year ago. Although lower doses worked in many patients, we found that this was often the wrong economic consideration, as disease recurrence at the end of treatment and the development of viral resistance during treatment appear to be related to insufficient initial dosing. So we have learned to be more aggressive from the beginning, which is cheaper in the long run (ie 2nd therapy is not required)
Our greatest experience is with remdesivir. This drug is expensive and the owner has to commit to a costly treatment process that takes 3 months. For most clients, this represents an emotional and financial burden. My view is that in many cases it is better to spend money on antiviral therapy as such than on extensive diagnostics and monitoring.

One of the approaches in newly diagnosed cats with severe disease is hospitalization of cats during the first 3-4 days of treatment. Patients begin treatment with remdesivir when receiving IV fluid therapy (typically 2-4 ml / kg / hr; first day Hartmann's solution or Plasmalyte followed by 0.45 % NaCl and 2.5 % dextrose containing 20 mmol KCl / l). On the 1st day of hospitalization, remdesivir is administered in a high dose intravenously (10-15 mg / kg diluted in 10 ml with saline and is given SLOWLY for 20-30 minutes or longer, manually or by infusion pump; in human patients, administration lasts 2 hours. ) to achieve an increased starting dose of drug distribution volume. This achieves fast antiviral efficacy. In cases with CNS disease, we recommend a daily IV dose of 20 mg / kg. Many cats may appear slightly depressed several hours after IV remdesivir infusion. In human patients, remdesivir may cause infusion-related reactions, including low blood pressure, nausea, vomiting, sweating or chills, but we have not observed these events in our feline patients.
The advantage of starting treatment intravenously is that dehydration, if present, is corrected and you have IV access if you need to take other medicines (eg anticonvulsants, corticosteroids). Importantly, once an IV catheter is inserted, daily injections of remdesivir do not cause any pain or discomfort. However, if the cat eats and is diagnosed in the early stages of the disease, then IV therapy is not required and the same doses can be given subcutaneously, saving a lot of money.
FIP cats treated with remdesivir typically improve significantly during the first 2-3 days. However, we found that cases of effusion, and especially those that resulted in pleural effusion prior to treatment, should be closely monitored, as the combination of the antiviral effect of remdesivir and a higher than maintenance dose of crystalloids may lead to transient worsening of pleural effusion. This requires drainage twice a day using a 19G butterfly needle (1.1 mm - cream color) and a 3-way stopcock (ideally using an ultrasonic guide to find the best place to insert the needle). These "secondary" pleural effusions can be fatal if not detected in time and appear to occur in approximately 1 in 10 cases of effusive FIPs treated with remdesivir.
Another problem that occasionally occurs at this time is the development of neurological symptoms, including seizures. Our view is that this is not the effect of the drug as such, but rather the unmasking of the subclinical CNS FIP. Such cats require careful monitoring, while the development of seizures requires the use of anticonvulsant drugs such as midazolam (0.3 mg / kg IV), alfaxane or propofol (administered IV to be effective), followed by levetiracetam (Keppra) (10- 20 mg / kg, PO every 8 hours). Phenobarbitone is a reliable anticonvulsant, but it tends to increase the metabolism of many drugs, and levetiracetam is probably safer until we better understand the pharmacokinetics and metabolism of remdesivir and GS-441524. Some doctors also administer dexamethasone or prednisolone as a single treatment to relieve CNS inflammation.
Although advocating initial IV therapy for the most severe cases of FIP, cats and kittens that are still "happy" and eating do not require IV therapy at first and may instead begin subcutaneous injections at 10-12 mg / kg / day (20 mg / kg in CNS diseases). This is, of course, much cheaper because cats or kittens do not have to be placed in an infusion pump and hospitalized in a stressful environment. For clients who have financial limits, this may be a more appropriate way to start therapy. Some skilled colleagues, such as Jim Euclid, have developed a hybrid approach where kittens receive subcutaneous fluids daily as a bolus with injected remdesivir.
The cats were then given continuous subcutaneous injections of remdesivir. It originally took 84 days, and such cases accounted for most of the cases we have dealt with so far. Recently, we have been using aggressive IV / SCI remdesivir for initial therapy, and then cats are switching to oral GS-441524 for 10 weeks of consolidation therapy.
After the initial use of lower doses, which were not successful in every patient, we now use the following treatment protocols:
- for cats with wet FIP: 10-12 mg / kg once daily (SID) for 2 weeks
- for cats with severe eye impairment: 15 mg / kg SID by subcutaneous injection (SCI) for 2 weeks; Cats with severe uveitis should also be given topical corticosteroids (Before Forte or Maxidex) for 2-3 days (no longer!) and atropine eye ointment.
- for cats with neurological FIP with CNS symptoms: administer 20 mg / kg SID SCI for 2-4 weeks. 5
It is important that owners are properly instructed on how to optimally administer daily injections. Cats will perceive the injection as less painful if the remdesivir solution in the syringe is allowed to warm to room temperature instead of being refrigerated. In addition, if you teach them simple tasks such as using a new needle when injecting (ie use a needle other than the one used to draw the medicine from the vial) and using 21G (0.8mm - green) or 23G diameter needles (0.6mm - blue), injections will be more tolerable. Although 21G needles are larger, some cats may have the advantage of injecting faster. Alternatively, for simplicity, veterinarians can prepare injections for the whole week, which they will keep in the refrigerator, and will give a new injection every day.
For cats that continue to perceive SC injections as painful, we used gabapentin orally (50 to 100 mg per cat) and / or transmucosally or SC administered buprenorphine 30-60 minutes before sedation / analgesia injection. The area to be injected can also be trimmed so that a topical EMLA cream can be applied 30 minutes before the injection. BOVA produces a faster-acting local anesthetic gel that may be useful in some patients. In exceptional cases, we inserted a cephalic catheter every 4-5 days so that owners could administer IV therapy instead of SC injections. Injection site reactions reported with GS-441524 injected abroad do not appear to occur with remdesivir.
After 2-4 weeks of taking remdesivir and after the abdominal fluid has disappeared and the ocular and CNS symptoms have improved or disappeared, we are now proposing a switch to GS-441524 tablets. This is done for 3 reasons: (i) it reduces costs (ii) eliminates the pain problem of SC injections (iii) in some patients it is more effective. Remdesivir injections are probably more reliable than oral GS-441524, and in the worst cases, you might choose to give them for 4 weeks, but for most cats, 2 weeks and comfort and lower oral formulation costs outperform everything else.
The use of GS-441524 tablets is relatively new in Australia but is widely used overseas. The recommended oral dose of GS441524 is generally the same as the SCI/IV dose of remdesivir: wet FIP cases receive 10-12 mg/kg PO SID, ocular cases 15 mg/kg PO SID and CNS cases 20 mg/kg (or higher). GS-441524 is more economical and is even safer than remdesivir. In CNS cases where large doses are given, it is probably best to give 10 mg/kg PO every 12 hours (BID) to circumvent the “ceiling” effect that has been reported in relation to limited absorption of high doses.

Why are the dosages about the same? At mg / kg, GS441524 has twice as many active molecules as remdesivir (due to the difference in their molecular weight), but the bioavailability of GS-441524 is only 50 % (only half of what is given is absorbed, and this is affected by feeding and also the effect of the ceiling dose) - so these two factors cancel each other out.
We recommend that GS-441524 tablets be given with a small treat to mask the tablet, with the main meal being served 1 hour later. The tablets provided by BOVA are 50 mg tuna-flavored tablets, with four score lines, so they can be divided into halves or even quarters.
In situations where owners cannot afford full treatment, we use mefloquine (Lariam; 5 mg / kg orally once daily in capsules or 62.5 mg twice a week) after initial treatment with remdesivir / GS-441524.
Phillip McDonagh, Jacqui Norris, Merran Govendir and colleagues at the Sydney School of Veterinary Science have shown that mefloquine has an antiviral effect. 7 This is probably due to the fact that mefloquine usurps the biochemical intracellular pathways used by the FIP virus, a mechanism that has recently been demonstrated with clofazimine. 8 (anti-leprosy medicine), and several other medicines. In several cats, where owners could not afford a complete treatment with remdesivir, mefloquine proved to be effective in reaching the limit of clinical cure.
The main advantage of buying remdesivir and GS-441524 from BOVA for the treatment of FIP cases is that the products we use are subject to quality control. It's just a prescription with the client's name and address, the patient's name and the dose to be given, and the compounder can usually deliver the vials or tablets to any veterinarian in Australia within 24-48 hours.
At present, the price is 100 mg of vials of remdesivir 250$ plus GST and postage (the total price is usually about 280$). GS-441524 is sold in packs of 10 tablets for 600$ plus shipping and handling. By purchasing more vials and tablets at the same time, of course, postage and handling fees will be reduced. We believe that most owners will feel much more comfortable getting a product from a well-known Australian company than sending money overseas and hoping that drugs of unknown quality on the black market will reach Australia safely without being detained by customs.
There is no reason why a well-motivated veterinarian would not be able to handle these cases in his own practice. This is often more convenient for the owner, especially if they struggle with daily injections and need a practice near them.

Veterinarians who wish to explore this option or have general questions about FIP case management may email Sally Coggins (dr.sallyc@gmail.com), Richard Malik (richard.malik@sydney.edu.au), David Hughes (concordvets@concordvets.com.au), Grette Howard (drgretta@gmail.com) or Professor Jacqui Norris (jacqui.norris@sydney.edu.au), for advice on diagnosis or treatment. Many Australian veterinarians interested in FIP have gained considerable expertise in the management of these cases. For example, Andrew Spanner in Adelaide treated more than 20 cases with excellent results. Thus, there are already many feline medicine physicians and internal medicine specialists with experience in the treatment of FIP, and so veterinarians who are hesitant to treat their own cases have the opportunity to recommend these specialists to their clients.
Physicians who accept FIP cases from GPs include: QLD Rhett Marshall, Marcus Gunew, Alison Jukes, Rachel Korman; NSW Katherine Briscoe, Michael Linton, Randolph Baral, Melissa Catt; VIC - Carolyn O'Brien, Keshuan Chow, Amy Lingard; WA-Martine Van Boeijen and Murdoch University Veterinary Hospital; TAS Moira van Dorsselaer.
All of these doctors (and probably even more we don't know about) are happy to accept cases for diagnosis and therapy. Everyone is probably happy to discuss case management with you.

Sally Coggins, working with Lara Boland, Emily Pritchard, Associate Professor Mary Thompson and Professor Jacqui Norris at the Sydney School of Veterinary Science, is interested in treating cases with comprehensive diagnosis and free monitoring. It will be part of Sally's doctoral program, so you will help her advance in her studies by sending her cases. We hope that through these studies, we will get a better idea of how quickly cats respond and when exactly treatment can be safely stopped. Owners will only have to pay for remdesivir and GS-441524 for therapy. This group is also interested in treating cases with interferon-omega and mefloquine.
In most cases, FIP is doing very well with GS-441524 or remdesivir. Niels Pedersen has gathered an amazing resource for veterinarians interested in FIP case management - https://sockfip.org/dr - pedersen - research / . The site also provides some recommendations on how to monitor cats during treatment. I'm not very protocol-oriented, so the key things for me to keep track of are appetite, attitude, activity levels, and changes in body weight and fitness over time. Most physicians like to monitor serum hematology and biochemistry every month to ensure that all measurable abnormalities improve, although this can be stressful for the patient and increase treatment costs. The trade-off is taking a few drops of blood to monitor PCV, total plasma protein (TPP) using refractometry, and plasma color to determine if anemia is improving, jaundice is subsiding, and gamma globulin levels are lowering, resulting in lower TPP.
Do not worry about transient increases in globulin levels at the start of treatment; when high protein effusions are absorbed, a lot of immunoglobulins enter the patient's plasma. This phenomenon may be common until the 8th week of treatment, but disappears by the 12th week.
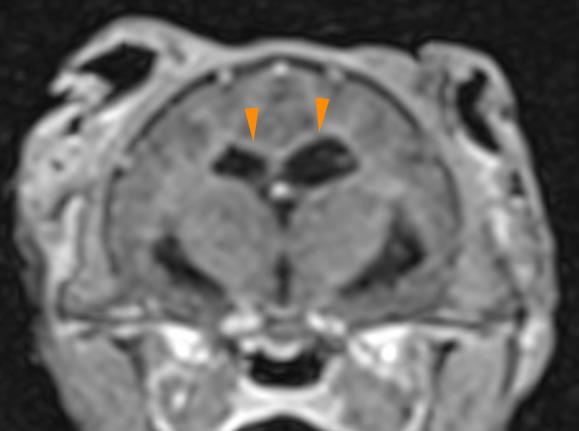
And what about a kitten with multifocal CNS disease, where FIP CNS is the most likely cause of clinical symptoms? The traditional approach is serology (to rule out cryptococcosis and toxoplasmosis), a good history and thiamine test to rule out vitamin B1 deficiency, followed by MRI scans (Figure 9) and CSF collection for fluid analysis and multiplex neuro-qPCR analysis). This approach is very expensive and there is also a certain risk of anesthesia and especially CSF collection. We found that a 3-5 day intravenous or sc. Remdesivir therapy can be used as a therapeutic test in cats with probable CNS FIP and is a cost-effective alternative to complete diagnostic processing, which can cost 3-5000$ or more.
Similarly, if exploratory laparotomy, abnormal tissue biopsy, histology, and immunohistochemistry for FIP antigen are used to diagnose dry intra-abdominal FIP versus 3-5 days of treatment with remdesivir or GS-441524, a drug test may be considered, which is a better choice from in terms of patient well-being and reduced costs. Most cats with non-fusive FIP experience rapid improvement with antiviral therapy, with normalized fever, improved appetite, and better overall attitude within 2 to 3 days. If the patient does not respond to antiviral therapy, then exploratory laparotomy and representative organ biopsy are reasonable, as the main differential diagnoses are lymphoma and lymphocytic cholangitis.
This is a matter of personal approach for each doctor. FNA for cytological and sometimes immunohistochemical examination or PCR is a convincing non-invasive option where this expertise is available, but sometimes it does not give a definitive answer. Some veterinarians insist on tissue diagnosis and positive immunohistology or PCR in each patient, while others would like to "treat treatable" with a 3-5-day remdesivir / GS-441524 application and proceed to exploratory laparotomy only when there is no clear response to therapy.
It is incredibly satisfying to see the transformation of cats and kittens, which are not well, into normal and happy cats. It's really something that will lift your spirits as a doctor. It's good science and good veterinary medicine!
Conclusions
In the past, the diagnosis of FIP was an intellectual exercise so that we could end the suffering of a cat or kitten with the certainty of an accurate diagnosis. Now, thanks to FIP's lifelong study, Dr. Niels Pedersen, we are able to successfully treat perhaps 80 % or more cats with FIP if the client has sufficient funds. It is too early to predict whether or how many will be repeated later.
There is a need for intensive study in diagnosis and case management, but with the necessary effort, a good veterinarian should be able to work with a determined owner to achieve a clinical cure. The most important thing is not to put too many obstacles in the way of the dedicated owner and support him during the 12-week marathon treatment course by helping him find the best way to treat his patient. This may include sedative / analgesic treatment to help the cat improve controllability and prevent discomfort when the client brings their cat to the clinic daily for remdesivir injections or switching to GS-441524 tablets when the stress from the injections is too great for the owner. It is important to go a long way and a payment plan can be provided that will allow determined clients to improve the affordability of treatment.
Finally, the impact of COVID-19 on coronavirus research has been indeed profound, and several very promising drugs are under development, such as molnupiravir from Merck and another oral drug from Pfizer.
OVERALL SUMMARY
2-step approach to therapy
Phase 1 - INDUCTION
IV / SC injections of Remdesivir
- For cats with wet FIP: 10-12 mg / kg remdesivir by subcutaneous injection (SCI) once daily (SID) for 2 weeks
- For cats with eye: 15 mg / kg SID remdesivir SCI for 2 weeks
- For cats with neurological symptoms of FIP and CNS: remdesivir 20 mg / kg SID for 2 weeks
Phase 2 - CONSOLIDATION
Switch to GS-441524 tablets after 2 weeks of remdesivir injection
- For cats with wet FIP: 10-12 mg / kg GS-441524 oral SID for 10 weeks
- For cats with eye impairment: 15 mg / kg SID GS-441524 oral SID for 10 weeks
- For cats with neurological symptoms of FIP and CNS: GS-441524 10 mg / kg oral BID (20 mg / kg / day) for 10 weeks
References
- Kim, Y .; Liu, H .; Galasiti Kankanamalage, AC; Weerasekara, S .; Hua, DH; Groutas, WC; Chang, KO; Pedersen, NC Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog. 2016, 12, e1005531.
- Pedersen, NC; Kim, Y .; Liu, H .; Galasiti Kankanamalage, AC; Eckstrand, C .; Groutas, WC; Bannasch, M .; Meadows, JM; Chang, KO Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392.
- Murphy, BG; Perron, M .; Murakami, E .; Bauer, K .; Park, Y .; Eckstrand, C .; Liepnieks, M .; Pedersen, NC The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233.
- Pedersen, NC; Perron, M .; Bannasch, M .; Montgomery, E .; Murakami,
E .; Liepnieks, M .; Liu, H. Efficacy, and safety of the nucleoside analog GS441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. - Dickinson PJ, Bannasch M, Thomasy SM, et al. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. Journal of Veterinary Internal Medicine. 2020. doi: 10.1111 / jvim.15780.
- Tasker S. Diagnosis of feline infectious peritonitis: Update on evidence supporting available tests. Journal of Feline Medicine and Surgery.
2018; 20 (3): 228-243. doi: 10.1177 / 1098612X18758592 - McDonagh, P .; Sheehy, PA; Norris, JM Identification, and characterization of small molecule inhibitors of feline coronavirus replication. Vet. Microbiol. 2014, 174, 438–447.
- Yuan, S., Yin, X., Meng, X. et al. Clofazimine broadly inhibits coronaviruses including SARS-CoV-2. Nature (2021).
https://doi.org/10.1038/s41586-021-03431-4 - https://sockfip.org/ - THE BEST resource on the internet or anywhere for FIP.

COSTS:
2 kg kitten with wet FIP
4 × 100 mg remdesivir vials - 1000$
35 × 50 mg tablets GS-441524 - 2100$
Manipulation and GST - 30$ plus 310$ = 340$
A total of 3440$, approximately 290$ per week for 12 weeks
4 kg cat with dry FIP
7 × 100 mg remdesivir vials - 1750$
70 × 50 mg tablets GS-441524 - 4200$
Handling and GST 30$ plus 600$
A total of 6550$, about 545$ per week for 12 weeks