As the name suggests, this is not about FIP, but it's important to know. I registered the strange information that when treating FIP with molnupiravir, it was also possible to cure FIV. And that cats that were positive before treatment were negative for FIV after treatment. And that the tests were not quick tests, but tests from Laboklin...
Apparently, many of you have the misconception that if something comes from a lab, that automatically means there is a clear answer. But it is a huge mistake. Let's talk about the principle of FIV and FeLV testing. Rapid tests (snaptests) are antibody-based for FIV and antigenic for FeLV. And here is the basic stumbling block. Antibodies, even if there is some miraculous cure, do not disappear after treatment. Antibodies are proteins produced by the immune system and their purpose is to identify and neutralize foreign objects in the body. So the very negative result of the proilase test after the treatment, before which the test was positive, means only one thing - One of the two tests was false positive (or false negative) and therefore defective.
It is for this reason that it is strongly recommended, especially in the case of a positive FIV or FeLV test, to perform a confirmation test using another laboratory method.
And why did I say that the fact that something is done in the laboratory does not necessarily mean anything? Simply. If you have the FIV and FeLV test done by a laboratory and do not specify the method, it is very likely that the laboratory will do a SNAP test or an ELISA (EIA) test. You can tell by the price of the test, but also by what is on the report. The image below shows that this was a test FIV AK, but what does it mean? antibody test (AK=Antikörper). In parentheses is EIA, which is an abbreviation for "enzyme-linked immunosorbent assay'. The abbreviation ELISA is also used. You should know that the gold standard of the confirmation test for FIV is the method test Western Blot... In that case, it would be mentioned in the report like this. Although the WB test is also an antibody test, it works on a completely different principle. For FeLV, the standard PCR is used as a confirmatory test. And something else. Why do you think you will test positive for FCoV antibody after treatment for FIP? Exactly for the reason I wrote about above. Antibodies remain in the body after treatment for FIP and this is completely natural. Even after you are cured of the much-maligned Covid, you will still have antibodies. Otherwise, it would be very bad for you. And ask yourself why FCOV antibodies would remain after treatment and FIV antibodies would disappear? Antibodies remain in the body for several months after treatment, and in some cases or for incurable diseases such as FIV, even for years.
In the picture you can see an FIV antibody test with a negative result, which led the cat's owner to the fantastic but unfortunately premature conclusion that the FIV was cured by treating the FIP.
For the sake of completeness, I am also attaching an FIV test using the Western Blot method for my cat, which unfortunately confirmed that it is FIV positive. And we even had a few snap tests done before (one even in the laboratory), some of which were negative and some were positive.
Please stop jumping to conclusions and tame the euphoria about the FIV cure. The result of two antibody tests with a conflicting result does not mean that a cure has occurred, but that one of the tests showed a faulty result.
In addition to the above information, you should also be aware that after vaccination based on the principle of an inactivated virus, it is no longer possible to use antibody tests for the diagnosis of the given disease, because the vaccination serves precisely to make the body create antibodies.
Antibody tests can come out positive even in the case of young kittens (under 20 weeks), when they can have maternal antibodies from breast milk and subsequently the tests can be negative.
Regarding PCR testing for FIV, I would add that you should read the article https://www.fivcats.com/FIV/fiv_testing.html, where the basic principles of FIV tests and their reliability are presented. You will learn, for example, that the error rate of negative PCR tests is really very high.
FIV treatment ???
The FIV virus is a retrovirus related to the virus that causes HIV (AIDS). The main problem is that the virus is "built" into the host genome and that is why such a disease is not treatable. Of course, this does not mean that the lifespan of the affected individual cannot be extended with the use of symptomatic therapy. If an FIV cat is affected by an infection, antivirals can help, if a bacterial infection appears, ATB is used... So, concomitant diseases and infections are addressed, and this treatment keeps the FIV disease itself under control, but it does not cure it. To be sure, I also asked those who are actually qualified about the possibility of treating FIV with molnupiravir. Answers from Danielle-Gunn Moore - professor of feline medicine at the University of Edinburgh and Yunjeong Kim - professor at Kansas State University, who, together with Dr. Pedersen is behind the discovery of the treatment of FIP with GS-441524, hopefully they will convince those who got "drunk" with the croissant and succumbed to the vision of treating FIV with molnupiravir.
Translation: "Retroviruses like FIV or HIV (AIDS) are not treatable with antivirals because the viruses are embedded in the host genome. If there is a good antiviral for FIV, it may help the cat stay symptom-free for a longer period of time (similar to HIV drugs in humans), but I don't think there is evidence that molnupiravir is effective against FIV."
Translation: "It was emphasized to me that molnupiravir, because it acts on a replicating virus, will never cure FIV, similar to the effectiveness of these drugs for HIV, because the proviral non-replicating virus can never be their target. Even for HIV, 3-4 drugs are always needed, occasionally 2 - just to keep it under control, so there really is no chance of a cure."
I am pleased to announce that I have ended my advisory role with SOCKFIP and have officially become a member of the SOCKFIP Board of Directors. This reflects my transition from academic to private life, but it will not affect my commitment to FIP research. I hope that this more direct involvement will help SOCKFIP transition to a broader role in feline health issues beyond FIP. FIP research continues at the University of California, Davis, as well as at other institutions around the world. FIP research projects at UC Davis are summarized in “ Best regards SOCK FIP" of 2022. SOCKFIP continues to provide financial assistance for such studies through public donations, and I will provide scientific expertise whenever needed.
I wish there was a licensed antiviral treatment for FIP in cats, but even the efforts of many individuals and groups have not been able to change the current reality. Therefore, it is questionable whether legal antivirals for FIP will reach the market in the next 2 to 5 years, even if the obstacles are removed immediately. Fortunately, restrictions on the general use of closely related human medicines for COVID-19 are being eased worldwide, allowing them to be prescribed by all doctors and used more widely in the field. Full human approval allows their use in animals, provided the drug needed is derived directly from the actual human product. This would allow drugs made for humans, such as remdesivir and molnupiravir (EIDD-2801), to be used legally in animals, albeit at the cost of human drugs. The goal should still be for drugs specifically licensed for animals and available at a veterinary rather than a medical price.
More and more veterinarians are already helping owners with treatment. However, it still saddens me that some vets have not heard of effective treatments for FIP, believe that published treatment reports are bogus, or that obtaining drugs from unapproved markets is so scary that they can't even help with treatment once an owner buys it. I commend those veterinarians who accept the reality of treatment and work with owners and their cats with FIP.
The most significant discovery after GS-441524 is the use of molnupiravir (EIDD-2801) (Merck) as a second effective treatment for FIP. Molnupiravir is also extremely effective in treating cats that have developed resistance to GS-441524, which are the most common cats that develop neurologic FIP during or after treatment with GS-441524. Reports of its use in cats are just beginning to emerge and are being posted on the SOCK FIP website.
I believe that there are several areas of research that veterinary researchers should consider. One area concerns the safety and efficacy of EIDD-1931 (beta-d-N4-hydroxycytidine), which is the biologically active component of molnupiravir, just as GS-441524 is the active component of remdesivir. This orally administered drug has been the subject of research for almost half a century and should no longer be patent protected. Preliminary research at the University of California, Davis suggests that it may be even more effective and safer than molnupiravir. I also believe that the oral protease inhibitor (nirmatrelvir) component of Paxlovid (Pfizer) should be tested for non-ocular/non-neurological cases of FIP. Nirmatrelvir is broken down into a simple chemical modification of GC373, the active form of GC376. Paxlovid is widely available and can be easily prescribed by both pharmacists and doctors for general treatment of COVID-19. This should make it widely available for use by veterinarians. I also believe that further research should be pursued to find ways to limit FECV infection and to understand the factors that suppress the natural normal protective immunity against FECV mutants. At this point, it is clear that most healthy cats have strong natural and acquired immunity to FIP viruses. What is this immunity and how can this knowledge contribute to strengthening immunity against FIP?
Meagan Roy 1, Nicole Jacque 2, Wendy Novicoff 3, Emma Li 1,Rosa Negash 1 , Samantha JM Evans 1 *
Department of Veterinary Biosciences, College of Veterinary Medicine, The Ohio State University, Columbus, OH 43210, USA
Independent Researcher, San Jose, CA 95123, USA
Departments of Orthopedic Surgery and Public Health Sciences, School of Medicine, University of Virginia, Charlottesville, VA 22903, USA
* Author to whom correspondence should be addressed.
Academic editors: Alessia Giordano and Stefania Lauzi Pathogens 2022, 11(10), 1209; https://doi.org/10.3390/pathogens11101209 Received: 19/09/2022 / Revised: 9/10/2022 / Received: 19/10/2022 / Published: 20/10/2022 (This article is part of a special issue of Advances on Feline Coronavirus Infection)
Feline infectious peritonitis (FIP) is a complex and historically fatal disease, although recent advances in antiviral therapy have revealed treatment options. A newer therapeutic option, unlicensed molnupiravir, is used as first-line therapy for suspected FIP and as salvage therapy for cats that have persistent or recurrent clinical signs of FIP after treatment with GS-441524 and/or GC376. Treatment protocols for 30 cats were documented based on owner-reported data. 26 cats treated with unlicensed molnupiravir as rescue therapy were treated with a mean starting dose of 12.8 mg/kg and a mean final dose of 14.7 mg/kg twice daily for a median period of 12 weeks (IQR = 10-15). A total of 24 of the 26 cats were still living without signs of disease at the time of writing this report. One cat was euthanized after treatment due to persistent seizures and the other cat underwent retreatment due to relapse of clinical signs. Few adverse effects have been reported, with the most prominent - drooping ears (1), broken whiskers (1) and severe leukopenia (1) - occurring at doses above 23 mg/kg twice daily. This study provides proof of principle for the use of molnupiravir in cats and supports the need for future studies to further evaluate molnupiravir as a potentially safe and effective therapy for FIP.
Keywords: FIP; coronavirus; antiviral drug; EIDD-2801; black market
1. Introduction
Feline infectious peritonitis (FIP) is a complex and historically fatal disease caused by mutation of the ubiquitous feline enteric coronavirus (FECV) [1]. Recent advances in feline and antiviral medicine have revealed potential treatment options for FIP. The 3C-like protease inhibitor GC376 was the first targeted antiviral therapy used against this disease [2]. GC376 was highly effective in improving clinical signs of FIP in 19 of 20 naturally infected cats, but showed limited ability to manage long-term disease [2]. Pedersen et al. continued to investigate the antiviral compound GS-441524, a nucleoside analog and active metabolite of remdesivir (GS-5734). GS-441524 demonstrated superior ability to treat and control disease in naturally infected cats compared to GC-376, with 25 of 31 cats disease-free at the time of writing [3]. Since these discoveries, cat owners worldwide have obtained these mostly unlicensed drugs to treat their FIP cats with remarkably high success rates [4]. Legal FIP treatment is in high demand in the United States due to ethical and legal concerns regarding the unlicensed drugs GC376 and GS-441524. In addition, some cats with FIP have exhausted all current treatment options due to disease relapse and/or treatment failure after GS-441524, GC376 and/or combination therapy. Therefore, an effective and legal treatment option for FIP is urgently needed. In connection with the recent outbreak of SARS-CoV-2, a number of new antivirals have entered the market. Molnupiravir (EIDD-2801), manufactured by Merck, is currently available under an emergency use authorization (EUA) from the FDA for the treatment of COVID-19 in adults [5]. It is an oral prodrug of the nucleoside analog BD-N4-hydroxycytidine, which increases guanine to adenine and cytosine to uracil nucleotide transition mutations in coronaviruses [6]. This mechanism increases the rate of mutations above the accepted limit, which in turn inactivates the virus [7]. Molnupiravir has been found to be safe and well tolerated at doses up to 800 mg twice daily in patients with COVID-19 [8]. Some studies have reported significant reductions in hospitalizations and deaths in mild-to-moderate COVID-19 patients, although efficacy appears to be lacking in severe COVID-19 patients [7].
Because of molnupiravir's strong potential to treat other coronavirus infections, cat owners have begun using unlicensed molnupiravir (or its active metabolite EIDD-1931) purchased over the Internet to treat FIP. However, the use of molnupiravir for the treatment of FIP is currently not documented in any scientific literature. Unlicensed molnupiravir can be used as first-line therapy for suspected FIP, but also as rescue therapy to treat cats that have persistent or recurrent clinical signs of FIP after GS-441524 and/or GC376 therapy. The aim of this study is to document this use and provide proof of principle for molnupiravir as a potential treatment for FIP based on owner-reported data.
2. Materials and methods
The survey was conducted using the Qualtrics XM program (Qualtrics Version May-August 2022, Provo, UT, USA) under license from Ohio State University. The survey (Supplementary Data S1) was written in English and consisted of 94 multiple-choice and free-response questions asking about FIP diagnosis, clinical signs, initial therapy (used before molnupiravir), molnupiravir treatment, adverse events, duration of treatment, and remission time. The number of free-response questions was limited to limit recall bias. The survey also allowed owners to upload relevant documents (eg veterinary medical records and laboratory results). The survey was formatted using questions from previous studies to maintain consistency of language and style, as well as newly developed questions specific to the experience of molnupivir treatment. The logic of the survey dictated that some questions appeared only after a particular answer was selected, while others were skipped when a particular answer was selected. This conditional logic was used to reduce questionnaire completion bias and questionnaire fatigue. The survey took approximately 20-30 minutes to complete and could be saved and completed later if needed. This study was approved by the Ohio State University Institutional Review Board (Protocol No. 2021E0162).
The survey was distributed to participants individually by email and data were collected from June to August 2022. Participants were selected from a subset of owners seeking molnupiravir therapy for their cat with suspected FIP through popular FIP therapy and social media support groups. Inclusion criteria were surveys of cats suspected of having FIP based on veterinary diagnosis, failure to respond to initial therapy, or recurrence of clinical signs after completion of initial therapy other than molnupiravir (eg, GS-441524 or GC376) and completion of 8–10 weeks of oral molnupiravir therapy (or those who subsequently died or were euthanized during therapy). This study also included a small group of cats that received molnupiravir for 8-10 weeks as initial and sole therapy, which will be referred to as first-line therapy in the rest of this paper, when FIP is suspected. Exclusion criteria were surveys with incomplete data or cats not diagnosed with FIP by a veterinarian.
3. Results
3.1 Demographic data
A total of 80 potential participants were identified through a social media FIP support group and 37 invitations to complete the questionnaire were sent to those participants with available contact details. A total of 33 questionnaires were mailed and 21 participants were sent follow-up emails to obtain complete questionnaire data. Seventeen owners attached relevant documents to the submitted questionnaires and two additional owners sent relevant documents containing veterinary medical records, laboratory results and diagnostic images to the study email address. These submitted documents were used to document adverse reactions reported by one participant. One response was a refusal to participate. Two cases were excluded because the cats did not have a diagnosis of FIP from a veterinarian (one of them was reported to have been diagnosed based on the loss of a sibling due to FIP and the other was examined by a veterinarian who concluded that blood tests were not consistent with FIP). A total of 30 cats with suspected FIP were therefore included in this study, 4 of which had not received any treatment prior to molnupiravir administration. These four cats were included as a separate small cohort of first-line molnupiravir treatment. A flow chart of these cases is shown in Figure 1. The countries of origin represented were the United States (25), Germany (2), Poland (2), and Sweden (1). The sex/neuter status of the cats at the time of diagnosis was 40 % neutered males, 40 % spayed females, and 20 % intact males. The mean age at diagnosis was 9.7 months, with a range of 1 month to 6 years. The majority of cats were of mixed or unknown breed (70 %); These included seven purebred cats and two special crossbreeds (e.g., a Balinese-Ragdoll-Siamese cross). Responses that referred to the cat as "American Shorthair" or "American Longhair" were instead categorized as mixed breed, given the commonly reported confusion among American owners regarding the nomenclature of this breed.
Figure 1. This flowchart represents the number of cases in each treatment block.
Regarding comorbidities, feline leukemia virus was reported in only one cat and calicivirus was reported in one cat. Several cats also had a history of external and/or internal parasitic infections (3), conjunctivitis/ocular infections (2), and bacterial skin infections (pyoderma) (1). A total of 16 cats had neurological signs of FIP. Three cats had both neurological and ocular manifestations of FIP, and two cats had only ocular manifestations of FIP. Of the remaining cases, seven were effusive, while five cases were non-effusive. The full breakdown of FIP types is shown in Table 1.
Cat
Age at diagnosis (months)
Sex/castration status at diagnosis
Tribe
Previous medical conditions
Country of origin
FIP form
Duration of initial treatment (weeks)
Disease-free period
Second therapy
Duration of the second therapy (weeks)
Disease-free period
The third therapy
Duration of the third therapy (weeks)
Disease-free period
1
4
Male
European shorthair
parasitic infections, URI at an early age
Germany
neurological
injectable oral GS-441524
8
none
injectable and oral GS-441524
15
none
2
15
neutered cat
Burmese
none
Sweden
effusive, non-effusive, neurological
injectable GS-441524
12
less than 4 weeks
injectable GS-441524
14
17 days
oral GS-441524
5 weeks
none
3
9
neutered cat
British Shorthair
none
Poland
effusive, neurological, ocular
injectable GS-441524
13
less than 2 weeks
injectable GS-441524
12
more than 6 months, less than 1 year
4
5
neutered cat
Abyssinia
none
USA
effusive
injectable GS-441524
12
less than 2 weeks
injectable GS-441524
14
less than 4 weeks
5
4
neutered cat
Balinese/Ragdol mix
calicivirus, conjunctivitis, giardiasis, tapeworm, URI
USA
non-effusive
injectable GS-441524
13
less than 8 weeks
6
7
neutered cat
Siamese
none
USA
neurological
injectable and oral GS-441524, injectable GC, injectable and oral molnupiravir
12
none
7
7
neutered cat
American Shorthair
none
USA
non-effusive
injectable and oral GS-441524
5
none
8
6
neutered cat
American Shorthair/Siamese mix
tapeworm, FCoV
USA
effusive, neurological
injectable and oral GS-441524
5
none
9
4
neutered cat
Homemade mixed
broken pelvis
USA
effusive
injectable and oral GS-441524
14
less than 6 months
oral GS-441524
13
less than 4 weeks
oral GS-441524/injectable GC
6 weeks in combination then 6 weeks of oral GS
none
10
4
neutered cat
Homemade mixed
none
USA
effusive
injectable GS-441524
23
less than 4 weeks
11
72
neutered cat
Homemade mixed
FeLV
USA
non-effusive
oral GS-441524
12
less than 6 months
12
5
Male
Homemade mixed
none
USA
non-effusive, neurological, ocular
injectable and oral GS-441524
17
none
13
01.V
Male
Savannah
none
USA
effusive, neurological
injectable and oral GS-441524
24
less than 6 months
injectable and oral GS-441524
12
less than 4 weeks
14
4
neutered cat
Homemade mixed
Skin and eye infections, fleas
Poland
non-effusive, neurological
injectable GS-441524
12
less than 2 weeks
injectable GS-441524
17
less than 4 weeks
15
12
neutered cat
American Shorthair
none
USA
effusive
injectable GS-441524/GC
01.V
none
16
5
neutered cat
Homemade mixed
none
USA
effusive, neurological
injectable GS-441524
12
less than 4 weeks
17
4
Male
American longhair
none
USA
ocular
injectable and oral GS-441524, GC376
13
none
18
6
neutered cat
Homemade mixed
none
USA
effusive
injectable GS-441524
12
none
19
12
neutered cat
Homemade mixed
none
USA
non-effusive
injectable and oral GS-441524
12
less than 2 weeks
injectable GS-441524
12
none
20
6
neutered cat
Unknown
none
USA
non-effusive, neurological
injectable GS-441524
4
none
oral GS-441524
3
none
21
4
neutered cat
Norwegian forest
none
USA
neurological
injectable GS-441524
12
less than 6 months
injectable GS-441524
01.V
none
Molnupiravir, GS-441524, GC
12 weeks
none
22
6
neutered cat
Homemade mixed
none
USA
neurological, ocular
oral GS-441524
3
none
23
12
neutered cat
Unknown
none
Germany
neurological
injectable GS-441524
16
less than 6 months
24
3
Male
Homemade mixed
none
USA
neurological
injectable GS-441524
12
less than 6 months
25
6
neutered cat
American Shorthair
none
USA
effusive
oral GS-441524
13
less than 1 week
26
1
Male
Unknown
none
USA
non-effusive
injectable GS-441524
12
less than 1 week
27
7
neutered cat
Homemade mixed
none
USA
non-effusive, neurological
Molnupiravir
12
less than 1 week
*Molnupiravir
28
24
neutered cat
Homemade mixed
none
USA
effusive
Molnupiravir
29
12
neutered cat
Homemade mixed
none
USA
non-effusive, ocular
Molnupiravir
30
24
neutered cat
Homemade mixed
none
USA
neurological
Molnupiravir
Table 1. Signaling and initial therapy characteristics of all 30 cats treated with unlicensed molnupiravir for suspected FIP.
3.2. Initial treatment before initiation of molnupiravir
A total of 26 of 30 cats received initial treatment for suspected FIP with unlicensed GS-441524 or a drug combination containing unlicensed GS-441524 as the main base drug (GS-441524-based). Half (13) of the cats were treated with injectable GS-441524. Only three cats were treated with oral GS-441524, while the other seven cats were treated with a combination of injectable and oral GS-441524 throughout the treatment period. Two cats were treated with a combination of the unlicensed drug GS-441524 and the unlicensed drug GC376. Cube no. 6 was treated with all previously mentioned drugs along with molnupiravir for 12 weeks of a very complicated regimen (Supplementary Data S2). Dosing of combination drugs used as part of primary therapy (eg, GC376 and molnupiravir) was not determined. Reported initial doses of the unlicensed GS-441524 ranged from 2 mg/kg to 10 mg/kg; the most frequently reported dosages were 5-6 mg/kg (eight cats) and 10 mg/kg (seven cats). Most (21) cats received a dose once a day. Only four were dosed twice daily, and one cat was dosed twice daily for one week at first, then switched to once daily dosing. The median duration of treatment based on GS-441524 was 12 weeks (IQR = 12-13). In fifteen cats, a change in daily doses was reported during treatment. For several cats, the daily dose was increased by body weight to maintain the same dosage in mg/kg. Others increased the mg/kg dosage because of insufficient clinical response or a change in route of administration (eg, from injectable to oral GS-441524). No participant reported dose reduction during treatment.
A total of 6 of 26 cats completed a shorter than average 12-week treatment with GS-441524 due to insufficient clinical response and were immediately started on another treatment. Two of the six cats initiated a different route or dose of unlicensed GS-441524 treatment as shown in Table 1. One cat switched from injectable to oral GS-441524 treatment on the second treatment. In the second cat, the dose of GS-441524 was simply increased during the second treatment. The remaining four cats started treatment with unlicensed molnupiravir at this time, as shown in Table 2. Of the 20 cats that completed at least 12 weeks of treatment with GS-441524, 16 experienced clinical remission. All 16 were in remission for less than 6 months, with 2 cats in remission for less than a week before clinical signs returned. All 16 started a second round of treatment, with 10 receiving a second round of GS-441524-based treatment and 6 starting molnupiravir at this time. Four cats that completed treatment with GS-441524 but did not achieve clinical remission were immediately started on molnupivir. A total of 26 cats received primary treatment with GS-441524 and all 26 relapsed or did not respond adequately. A total of 10 of 26 completed a second round of GS-441524-based treatment and 16 started molnupivir treatment.
Cat
Clinical symptoms at the beginning of treatment
Brand name
Initial dosage and frequency
Final dosage and frequency
Duration of treatment (weeks)
Time to improve
Persistent clinical symptoms
The result
Adverse effects
1
diarrhea, vomiting
Aura Plus
11 mg/kg twice daily
11 mg/kg twice daily
12
less than 1 week
none
clinical remission
none
2
none reported
Aura
12 mg/kg twice a day
12 mg/kg twice a day
12
uncertain
none
clinical remission
none
3
anisocoria, colored spots in the eye, polydipsia, pica, weight loss
Aura 2801
28 mg/kg twice daily
14 mg/kg twice a day
12
within 2 weeks
none
clinical remission
none
4
anorexia, lethargy, weight loss
EIDD
7 mg/kg twice a day
7 mg/kg twice a day
12
less than 1 week
none
clinical remission
none
5
colored spots in the eye, diarrhea, hiding and lack of socialization
Aura 2801
6 mg/kg once daily
13 mg/kg once daily
10
within 2 weeks
none
clinical remission
none
6
anisocoria, constipation, anorexia, fecal and urinary incontinence, lethargy, paralysis, seizures, pale gums, weight loss
Aura 2801
20 mg/kg twice a day
20 mg/kg twice a day
11
less than 1 week
none
clinical remission
none
7
anorexia, difficulty walking, hiding, lack of socialization, jaundice, lethargy
anorexia, heavy walking, hiding, lack of socialization, lethargy, unusual timidity
Aura 2801
11 mg/kg twice daily
16 mg/kg twice a day
18
more than 4 weeks
nothing physical but the MRI is still not normal
clinical remission
none
15
blindness, constipation, anorexia, diarrhea, enlarged abdomen, hiding, lack of socialization, lethargy, pale gums, weight loss
Aura 2801
16 mg/kg twice a day
16 mg/kg twice a day
12
less than 1 week
none
clinical remission
none
16
anorexia, difficulty walking, lethargy, seizures, tremors, weight loss
Aura 2801
14 mg/kg twice a day
14 mg/kg twice a day
12
less than 1 week
none
clinical remission
none
17
cough, anorexia, difficulty breathing, hiding, lack of socialization, lethargy, vomiting, weight loss
Aura 2801 and Aura 1931
12 mg/kg twice a day
17 mg/kg twice a day
20
within 3 weeks
anorexia
clinical remission
nausea/vomiting, anorexia
18
constipation, anorexia, difficulty walking, hiding, lack of socialization, weight loss
Aura 2801
12 mg/kg twice a day
12 mg/kg twice a day
8
within 2 weeks
none
clinical remission
none
19
lethargy, anorexia
Aura 2801
12 mg/kg twice a day
12 mg/kg twice a day
7
within 2 weeks
none
clinical remission
none
20
trembling/shaking
Aura 2801
10 mg/kg twice a day
23 mg/kg two to three times a day
10
less than 1 week
in remission about 1 1 weeks before the onset of seizures
euthanasia
decreased appetite when dosed three times a day, severe leukopenia, loss of beard, scaly skin on ears
21
difficulty walking, fecal incontinence
Aura 2801 and Aura 1931
13 mg/kg twice a day
30 mg/kg twice a day
14
less than 1 week
difficult walking, difficult jumping, fecal incontinence persisted during the study (1 week post treatment)
relapse and euthanasia
drooping ear tips, muscle weakness
22
colored spots in the eye, anorexia, difficulty walking, hiding, lack of socialization, lethargy
Aura 2801
16 mg/kg twice a day
19 mg/kg twice a day
9
within 2 weeks
none
clinical remission
none
23
difficulty walking, anorexia, loss of balance
EIDD aura
12 mg/kg twice a day
15 mg/kg three times a day
10
within 2 weeks
heavy walking
clinical remission
none
24
blindness, colored spots in the mouth, anorexia, difficulty breathing, difficulty walking, enlarged abdomen, urinary incontinence, jaundice, lethargy, paralysis, tremors
Aura 2801
15 mg/kg twice a day
15 mg/kg twice a day
16
less than 1 week
none
clinical remission
none
25
difficulty breathing, difficulty walking, hiding, lack of socialization, lethargy, URI
Aura 2801
7 mg/kg twice a day
7 mg/kg twice a day
16
within 2 weeks
none
clinical remission
none
26
lethargy, anorexia
Aura 2801
14 mg/kg twice a day
14 mg/kg twice a day
15
less than 1 week
neurological twitches, elevated liver enzymes
clinical remission
none
Table 2. Treatment and outcome characteristics of 26 cats receiving unlicensed molnupiravir as rescue therapy.
3.3. The second round of treatment before the initiation of molnupiravir
Overall, 10 of 26 cats that received initial GS-441524 treatment and subsequently relapsed were reported to have received a second round of unlicensed GS-441524 treatment prior to initiation of molnupiravir. Again, most cats received injectable GS-441524 (6), with two receiving oral GS-441524 and two receiving both injectable and oral GS-441524. Reported dosages ranged from 4-5 mg/kg to 15 mg/kg; the most frequently used dosages were 7-8 mg/kg (two cats) and 15 mg/kg (two cats). Most cats were dosed once daily (seven cats), one cat was dosed twice daily and one cat was dosed three times daily. In most cats, the dose was varied during treatment. The two doses were weight-adjusted to maintain the same dosage in mg/kg. Dosing in mg/kg was increased in five cats that did not respond adequately or developed new clinical signs (eg, neurological signs). The median duration of treatment was 12.5 weeks (IQR 9.75–14.25). Only two cats did not undergo at least 12 weeks of therapy. One of the two added GC376 and molnupiravir to current GS-441524 therapy, and the other started molnupiravir as sole therapy. Of the eight cats that completed at least 12 weeks of GS-441524 therapy, two did not achieve clinical remission. Both cats started treatment with unlicensed molnupiravir at that time. The remaining six cats were reported to achieve clinical remission after a second round of treatment with GS-441524. Five of the six cats were in remission for less than 4 weeks, with the exception of one cat that was in remission for more than 6 months but less than a year. Seven out of ten cats started taking unlicensed molnupiravir at this time.
3.4. The third round of treatment before starting molnupiravir
The remaining three cats received a final round of GS-441524-based treatment before switching to molnupiravir. Cat no. 2 received oral GS-441524 for 5 weeks prior to initiation of molnupiravir. Cat no. 9 was treated for 6 weeks with oral and injectable GS-441524 and then continued for 6 weeks with oral GS-442524 alone. Dosing and frequency in both cats are unknown, as the survey collected data on only two therapies prior to molnupivir. Cat no. 21 received a combination of GS-441524, GC376 and molnupiravir for 12 weeks. The dosage, frequency and duration of each varied radically over the course of 12 weeks (Supplementary Data S3). All three cats started treatment with molnupiravir without clinical remission from this third round of treatment.
3.5. Molnupiravir as rescue therapy
Of the 26 cats receiving unlicensed molnupiravir as rescue therapy, most were using the Aura brand, with only 2 cats using a different brand of molnupiravir. More than 81 % cats (18) were treated with Aura 2801, 1 cat was treated with Aura 1931, and another 2 cats were treated with both Aura preparations. The mean initial dosage was 12.8 mg/kg twice daily. One cat was dosed only once a day and two cats were dosed 2 to 3 times a day. The most commonly used initial dosage was 12 mg/kg twice daily. Dosage ranged from 6 to 28 mg/kg twice daily. 11 dosage changes were reported, all but one being an increase in dosage. Reduction of dosage in cat no. 3 was not explained in any way. The mean final dosage was 14.7 mg/kg twice daily, with the same three cats differing in dosing frequency. The most common final dosage was also 12 mg/kg twice daily. The dosage range was 7 to 30 mg/kg twice daily.
Median duration of treatment was 12 weeks (IQR 10-15). Overall, a wide range of 7-20 weeks was reported. Only eight cats were treated for less than 12 weeks. A cat that completed only 7 weeks of treatment was reported to have discontinued treatment due to achieving clinical remission. All 26 cats completed treatment at 7 weeks or longer and all 26 cats survived. No cases of missed doses of molnupiravir have been reported.
Owners reported improvement in clinical signs in more than 92 % cats within three weeks of initiation of molnupiravir treatment, with 84.6 % cats showing improvement within two weeks and nearly half (46.2 %) within one week. Only two cases were reported differently, with one cat showing no signs of improvement for up to 1.5 months, and the owner of the other cat being unsure of the timescale and degree of improvement in clinical signs. A total of seven cats with persistent clinical signs of FIP were reported. In one of them, the disappearance of clinical symptoms was reported after one week of the observation period. Others are thought to have had residual symptoms such as difficulty walking or jumping, tremors, MRI changes and fecal incontinence. The full range of persistent clinical signs is shown in Table 2. Only three cats reported adverse reactions in response to molnupiravir, including nausea/vomiting, anorexia, drooping ear tips (Figure 2), brittle whiskers, leukopenia, scaly skin and muscle wasting. At the time of publication, 24 of 26 cats are living in clinical remission of FIP after oral molnupiravir treatment. One cat reportedly died 1 week after discontinuation of molnupiravir due to a prolonged seizure, and the other cat (No. 21) was disease-free 4 weeks before relapse. Cat no. 21 then started a second round of molnupiravir at the same dose, but was subsequently euthanized due to insufficient response to treatment.
Figure 2. Dropped ear tips were reported as an adverse effect of unlicensed molnupiravir treatment in cat no. 21.
In cat no. Severe leukopenia was reported in 22 cases. Through veterinary records, it was found that cat no. 22 has moderate panleukopenia with lymphopenia, neutropenia, and normal hem and thrombograms on 4 of 5 sequential complete blood counts, which were confirmed through veterinary records of sequential complete blood counts. The initial white blood cell count recorded was 10,700 cells per microliter (reference range 3,500–16,000 cells per microliter). Four more complete blood tests showed white blood cell counts ranging from 1,200 to 1,900 cells per microliter. The initial neutrophil count was 8560 cells per microliter (reference range 2500-8500 cells per microliter). The other four neutrophil counts ranged from 696 to 1292 cells per microliter. The initial lymphocyte count was 1177 cells per microliter (reference range 1200-8000 cells per microliter). The other four lymphocyte counts ranged from 330 to 532 cells per microliter.
3.6. Molnupiravir as primary therapy
A small group of four cats were treated with unlicensed molnupiravir as sole therapy for suspected FIP, as shown in Table 3. Three of them reportedly chose molnupiravir over the unlicensed counterpart GS-441524 due to financial constraints. Cat no. 29 received 12 weeks of oral molnupiravir 12 mg/kg twice daily prior to the treatment shown in Table 3. This cat was disease-free for less than one week prior to restarting oral molnupiravir 19 mg/kg twice daily for 10 weeks.
Cat
Clinical symptoms at the beginning of treatment
Brand name
Initial dosage and frequency
Final dosage and frequency
Duration of treatment (weeks)
Time to improve
Persistent clinical symptoms
Conclusion
Adverse effects
* 27
Hiding, lack of socialization, lethargy, anorexia, URI, vomiting, weight loss
Aura 2801
19 mg/kg twice a day
19 mg/kg twice a day
10
less than 1 week
none
clinical remission
none
28
Anorexia, difficulty walking, distended abdomen, hiding, lack of socialization, lethargy
Aura 2801
8 mg/kg twice a day
8 mg/kg twice a day
13
in two weeks
none
clinical remission
none
29
Anisocoria, blindness, eye color changes, anorexia, hiding, lack of socialization, urinary incontinence, lethargy,
Aura 2801
10 mg/kg twice a day
10 mg/kg twice a day
13
in two weeks
none
clinical remission
none
30
Hiding, lack of socialization, lethargy, pale gums, weight loss
Aura 2801
10 mg/kg twice a day
12 mg/kg twice a day
10
in two weeks
none
clinical remission
none
Table 3. Treatment and outcome characteristics of 4 cats receiving unlicensed molnupiravir as primary therapy.* They received two rounds of molnupiravir treatment; the first round is documented in Table 1.
All four cats were treated with oral molnupiravir Aura 2801 at a mean starting dose of 11.75 mg/kg twice daily (range 8-19 mg/kg) and a mean final dose of 12.25 mg/kg twice daily (range 8-19 mg/kg ). The median duration of treatment was 11.5 weeks (IQR 10-13), with two cats treated for 10 weeks and two cats treated for 13 weeks. A Mann-Whitney test was performed and no significant difference was found between the median duration of molnupivir as rescue therapy (12) and the duration of molnupivir as initial therapy (11.5) (p = 0.692). All owners reported seeing clinical improvement within two weeks and one cat showed improvement within one week. All cats survived the treatment, were disease-free at the time of publication, and no adverse effects of the treatment were reported.
3.7. Molnupiravir by type of FIP
The above information was collected for all 30 cats and then further divided according to the clinical forms of FIP. First, 16 cats with a reported neurological form of FIP were evaluated. Subsequently, the other cats were divided according to ocular (2), effusive (7) and non-effusive (5) forms. The mean starting dose of molnupiravir in the neurological form of FIP was 14.4 mg/kg twice daily, with two cats treated 2-3 times daily. The mean final dosage was 16.4 mg/kg twice daily, with two cats treated 2-3 times daily. The most commonly used initial and final dosage was 12 mg/kg twice daily. Median duration of treatment for neurological FIP was 12 weeks (IQR 10-12,641).
In the two remaining cases of ocular FIP, the mean initial dose was 11 mg/kg twice daily and the mean final dose was 13.5 mg/kg twice daily. The treatment lasted an average of 16.5 weeks. Seven cases of effusive disease were treated with a mean initial dose of 10.5 mg/kg twice daily and a mean final dose of 11.1 mg/kg twice daily. Treatment lasted an average of 13 weeks (IQR 12–16). Five non-effusive cases were treated with a mean initial dose of 10.6 mg/kg twice daily and a mean final dose of 12.8 mg/kg twice daily. One cat was treated once a day. The average duration of treatment was 10 weeks (IQR 8.5-13.5).
3.8. Costs and owner satisfaction
The majority of cats in this study were switched to unlicensed molnupiravir due to treatment failure/relapse or insufficient response. In addition to cats that relapsed or did not respond to unlicensed GS-441524-based therapy, one cat did not tolerate the injectable form of GS, and three owners were restricted due to the cost of treatment. Owners were not required to disclose the financial cost of treatment; this information was provided on a voluntary basis only. In addition, “0” responses reported in the report were not included in the calculation of the following averages because it was not possible to distinguish whether “0” represented no cost or unknown cost. The average reported cost for the first round of GS-441524-based therapy was $3448.83, and similarly, the average reported cost for the second round of GS-441524-based therapy was $3509.09. Only 4 owners reported paying for molnupiravir treatment, while 16 others reported “0” (or no cost/cost unknown). The overall average for the 20 owners who responded to the survey question regarding financial costs (including “0” responses) for molnupiravir was $209. The average cost for the four owners who did not respond with a “0” response was $1045. While 90 % owners reported being “very” or “somewhat” satisfied with their experience of their cat’s molnupiravir treatment, three were “very dissatisfied” with their experience. Unfortunately, no explanation was provided for the reported dissatisfaction.
4. Discussion
In this work, we describe the first known use of unlicensed molnupiravir for the treatment of suspected FIP in cats based on owner-reported data. For the treatment of cats using unlicensed molnupiravir as primary therapy for suspected FIP, the combined data from this study suggests that dosing at 12 mg/kg twice daily for approximately 12 weeks is effective in achieving clinical remission. For the treatment of cats receiving molnupiravir as rescue therapy when failing or relapsing after GS-441524-based therapy, the combined data from this study suggests that dosing at 12-15 mg/kg twice daily for 12-13 weeks is effective in achieving clinical remission. However, when broken down by clinical form of FIP, it was found that neurological cases of FIP were generally treated with a higher dosage than the average for all types of FIP. Ocular, effusive and non-effusive cases were treated with a dosage of around 12 mg/kg twice daily, with some variations. Therefore, dosing of 15 mg/kg molnupiravir twice daily for 12 weeks appears to be effective for neurological cases of FIP. For ocular, effusive, and non-effusive cases, 12 mg/kg molnupiravir twice daily for 12–13 weeks appears to be effective.
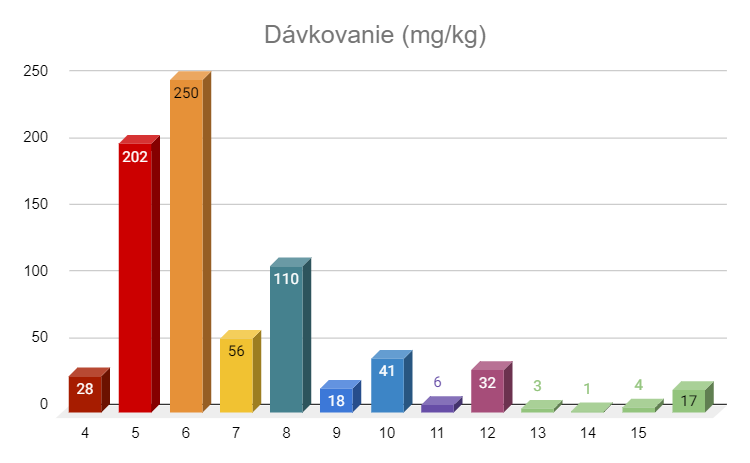
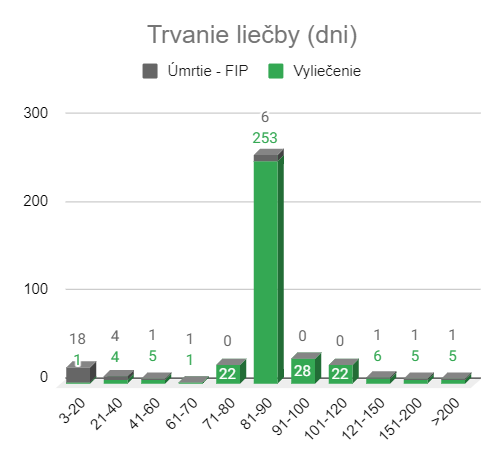
These data are somewhat inconsistent with the proposed treatment protocol of the company manufacturing the unlicensed molnupiravir under the trade name HERO Plus 2801. The recommended dosage in the package insert is 25 mg/kg once daily for effusive and non-effusive FIP, 37.5 mg/kg once daily for ocular FIP, and 50 mg/kg once daily for neurological FIP [9]. The package insert for HERO Plus 2801 also reports preliminary results from a study entitled “Effect of Oral Nutrition Therapy on Survival and Quality of Life in Feline Infectious Peritonitis,” which included 286 cats diagnosed with FIP. According to this package insert, 28 cats were cured after 4 weeks of treatment and 258 cats were cured after 8 weeks of treatment, with no deaths at the time of writing [9]. Data from this study have not yet been published in the scientific literature.
However, the cats in this study were using molnupiravir from a different supplier, Aura, which did not provide specific treatment recommendations. The treatment protocols used were therefore based on advice and information shared in groups on social networks, worksheets published on the Internet [10,11] and information on possible adverse effects contained in information published as part of human drug approval applications [12].
The molnupivir treatment protocol derived from this study more closely matches an independently designed protocol [10] published on the Internet. Based on data from in vitro cell cultures of EIDD-1931 and EIDD-2801, laboratory and field studies of GS-441524, and human pharmacokinetic studies, these authors extrapolated the effective dosage of oral molnupiravir [10]. Their calculations suggested a dosage of 4.5 mg/kg every 12 h for effusive and non-effusive FIP, 8 mg/kg every 12 h for ocular FIP, and 10 mg/kg every 12 h for neurological FIP [10]. Although the dosage in this study was generally higher than the dosage suggested by the cited authors, the high survival rate and low relapse rate at the time of the study termination suggest that the manufacturer's unlicensed recommendations may not represent the lowest effective dosage. Ultimately, controlled scientific experiments are greatly needed to evaluate the lowest effective dosage of molnupiravir in cats with suspected FIP.
Several cats were treated with Aura 1931, which is the active metabolite of molnupiravir, EIDD-1931. The reported dosages used were in a similar range to those reported for molnupiravir. Nominally, because the molecular weight of EIDD-1931 is lower than that of EIDD-2801, these cats received more active drug than cats using molnupiravir. However, a previous study showed decreasing oral bioavailability with increasing doses in mice. Therefore, the difference in bioavailability may not be proportional [13]. Pharmacokinetic studies of both molnupiravir and EIDD-1931 in cats are unfortunately unknown.
No adverse effects were reported in the package insert for HERO Plus 2801, which is contrary to what was reported in this study. Among the reported side effects of molnupiravir, the most prominent were drooping ears, hair loss, and severe leukopenia. No skin or follicular lesions have been reported in the human medical literature to match the whisker shedding or ear folding reported here. However, it should be noted that the cats that experienced these side effects received the two highest doses of molnupiravir shown in this study: 23 mg/kg three times daily and 30 mg/kg twice daily.
Severe bone marrow toxicity was reported in dogs during a 28-day study that was discontinued due to severe drug effects [12]. At the dosage of 17 mg/kg/day and 50 mg/kg/day, all hematopoietic cell lines were affected [12]. Cat no. 22 received a maximum dosage of 23 mg/kg three times daily, which was much higher than the toxic dosage in dogs of 17 mg/kg once daily. In the study group with a dose of 17 mg/kg, the possibility of reversibility was noted when the treatment was stopped [12].
There are concerns about the content of unlicensed brands of molnuviravir, as these brands are not currently regulated and often do not list the actual ingredients. The Hero brand (same manufacturer as HERO Plus 2801) shown in Figure 3 was analyzed by our group in December 2021 through Toxicology Associates Inc. (Columbus, OH). It was found to contain 97.3 % of molnupivirus, with no other contaminants detected. The Aura 2801 product used by the majority of participants in this study was analyzed in September 2022 by the same laboratory. It was found to contain 96.8 % of pure molnupivirus. A more controlled assessment of the actual content and purity of the unlicensed preparations of both GS-441524 and molnupiravir is of great interest to the veterinary community and is an active research topic in our group.
Figure 3. Images of Hero brand unlicensed molnupiravir packaging.
Some limitations of this study result from the retrospective nature and legality of the therapies used. First, all data used in this study were obtained based on owner reports. Working closely with the owners and administrators of the social media websites that supported this group enabled a better understanding and interpretation of many of the survey responses. Due to the lack of a definitive ante-mortem diagnosis of FIP available for practical use, it was also not possible to confirm that the cats included in this study had FIP. In addition, the data are likely to be biased toward positive outcomes and may be burdened by recall error. During the distribution phase, a potential study participant responded by requesting to be removed from our email list and stating that he did not wish to participate in the study. Their cat did not respond to molnupiravir treatment and was eventually euthanized. We assume that others may have had the same feeling, since three other potential participants did not respond to the invitation to the study. This may have narrowed the number of participants with an adverse outcome and falsely inflated apparent survival rates. Therefore, the data presented here are intended to serve as evidence of the feasibility of using molnupiravir as primary or rescue treatment for FIP, not as an indication of the true rate of efficacy.
In cats using unlicensed molnupiravir as rescue therapy, the cause of failure to respond or relapse after GS-441524-based therapy was not determined. It could be related to the quality of the drug, the resistance of the virus or another factor. As there is currently no testing or regulation in the US, unlicensed versions of GS-441524 or GC376 may be of insufficient purity or concentration, leading to treatment failure. Another possible cause is natural or acquired resistance to GS-441524. These two causes may also be linked, as acquired resistance may be promoted when an insufficient amount of antiviral is used in treatment, for example with low-quality drugs.
A recent paper found no drug-induced viral mutations of SARS-CoV-2 during molnupivir treatment [14]. This suggests that SARS-CoV-2 is unlikely to develop resistance to molnupiravir. Therefore, treatment with molnupiravir may be similarly unlikely to induce FIPV resistance, making it an attractive therapeutic option.
However, there is clearly a need for (1) a legal (in the United States and elsewhere) alternative to unlicensed treatment with GS-441524 and (2) the availability of alternative rescue drugs, either alone or in combination, after failure of GS-441524 treatment. Molnupiravir has the potential to fill both of these gaps, and this is the first known report of its use in cats in the literature. Nevertheless, unlicensed preparations may continue to be used for the treatment of FIP given the cost and the widely established networks available for their acquisition.
In conclusion, according to owner-reported data, unlicensed molnupiravir appears to be an effective treatment for suspected FIP, both as a first-line and rescue treatment. At a dose of 12–15 mg/kg every twelve hours, minimal side effects are reported and it provides a survival benefit with clinical resolution of FIP. Although the experiences of these owners in treating and possibly curing cats with FIP are unconventional and potentially illegal, they are undeniably remarkable and there is much to learn from the experiments these “citizen scientists” are conducting. In reporting these experiences, we aim to provide a basis for investigating molnupiravir for use in cats with suspected FIP and to document a phenomenon of “group health” that our profession should not ignore.
Supplementary materials
The following supplementary information can be downloaded at https://www.mdpi.com/article/10.3390/pathogens11101209/s1 Supplementary Data S1: retrospective review of molnupiravir trials; additional data S2: abbreviated diary of clinical history cat. no. 6; supplementary data S3: Cat #21 abbreviated clinical history log.
References
Felten, S .; Hartmann, K. Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature. Viruses2019, 11, 1068. [Google Scholar] [CrossRef] [PubMed]
Pedersen, NC; Kim, Y.; Liu, H.; Kankanamalage, ACG; Eckstrand, C.; Groutas, WC; Bannasch, M.; Meadows, JM; Chang, K.-O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg.2018, 20, 378–392. [Google Scholar] [CrossRef] [PubMed]
Pedersen, NC; Perron, M .; Bannasch, M .; Montgomery, E .; Murakami, E .; Liepnieks, M .; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg.2019, 21, 271–281. [Google Scholar] [CrossRef] [PubMed]
Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-Like Antiviral Therapy Can Be Effective for At-Home Treatment of Feline Infectious Peritonitis. Animals2021, 11, 2257. [Google Scholar] [CrossRef] [PubMed]
Merck & Co., Inc. Authorized for Emergency Use in the Treatment of COVID-19. Lagevrio. 2022. Available online: https://www.lagevrio.com/patients/ (accessed on 26 August 2022).
Gordon, CJ; Tchesnokov, EP; Schinazi, RF; Götte, M. Molnupiravir promotes SARS-CoV-2 mutagenesis via the RNA template. J. Biol. Chem.2021, 297, 100770. [Google Scholar] [CrossRef]
Singh, AK; Singh, A.; Singh, R.; Misra, A. Molnupiravir in COVID-19: A systematic review of literature. Diabetes Metab. Syndr. Clin. Res. Rev.2021, 15, 102329. [Google Scholar] [CrossRef] [PubMed]
Khoo, SH; Fitzgerald, R.; Fletcher, T.; Ewings, S.; Jaki, T.; Lyon, R.; Downs, N.; Walker, L.; Tansley-Hancock, O.; Greenhalf, W.; et al. Optimal dose and safety of molnupiravir in patients with early SARS-CoV-2: A Phase I, open-label, dose-escalating, randomized controlled study. J. Antimicrob. Chemother.2021, 76, 3286–3295. [Google Scholar] [CrossRef] [PubMed]
European Medicines Agency. Committee for Medicinal Products for Human Use (CHMP) Assessment Report: Use of Mol-Nupiravir for the Treatment of COVID-19. 2022. Available online: www.ema.europa.eu/contact (accessed on 8 October 2022).
Painter, GR; Bowen, RA; Bluemling, GR; DeBergh, J.; Edpuganti, V.; Gruddanti, PR; Guthrie, DB; Hager, M.; Kuiper, DL; Lockwood, MA; et al. The prophylactic and therapeutic activity of a broadly active ribonucleoside analog in a murine model of intranasal Venezuelan equine encephalitis virus infection. Antivirus. Res.2019, 171, 104597. [Google Scholar] [CrossRef] [PubMed]
Fletcher, T.; Ah Donovan-Banneld, I.; Penrice-Randal, R.; Goldswain, H.; Rzeszutek, A.; Pilgrim, J.; Bullock, K.; Saunders, G.; Northey, J.; Dong, X.; et al. Characterization of SARS-CoV-2 genomic variations in response to mol-nupiravir treatment in the AGILE Phase IIa clinical trial. Res. Sq.2022. [Google Scholar] [CrossRef]
The development of FIP treatment with GS441524 was such that, since its discovery, it started with the use of an exclusively injectable form, to which a tablet form of the drug was later added. However, the existence of two forms using the same active substance brought a bit of confusion, which is related to the difference in absorption (biological availability - usability) of the active substance during injection and oral use. While almost 100% of the drug is used during injection, it is only about 50% for GS when administered orally. In order to be able to use the same dosage for both injectable and tablet forms of medicine, most manufacturers who produce both forms of medicine list the so-called equivalent GS content, which already takes into account the reduced availability of the drug administered orally. In this way, it is possible to easily switch from injections to tablets and vice versa. So, for example, if a tablet from the well-known manufacturers Lucky, Spark, or Hero etc... is equivalent (corresponding to the injectable form) let's say 16mg of GS, in fact it contains double the amount of GS, i.e. 32mg... But we can safely use 16mg in the calculation and follow the dosage recommendations for injectable use. However, due to the fact that many different manufacturers want to grab their piece of the GS pie on the market, many of them often state the real GS content for marketing reasons, because of course such a tablet looks financially more attractive than a tablet with the stated equivalent GS content... For such tablets but you really have to to know for sure from the manufacturer, what GS content it actually states, because if it states, for example, 40mg real content of GS in the tablet, when calculating the dose according to the generally valid recommendations for injections, you only have to use half tablet content… In other words, you use a 40mg GS tablet in your calculations as a 20mg tablet…
At this point, I would like to emphasize that GS-441524 is proven and safe by clinical studies and hundreds of thousands of cured cats worldwide, with minimal side effects, and is therefore used as a medicine first choice.
Recommended approximate dosage of GS-441524 at injection application or for tablets with the stated equivalent containing GS441524. The stated dosage applies to 1kg / 24h:
6 mg/kg q24h – Wet FIP
8 mg/kg q24h – Dry FIP
10 mg/kg q24h – Ocular FIP
12 mg/kg q24h – Neurological FIP
15 mg/kg q24h – Neurological relapse
Recommended approximate dosage of GS-441524 for tablets with the stated real containing GS441524. The stated dosage applies to 1kg / 24h:
12 mg/kg q24h – Wet FIP
16 mg/kg q24h – Dry FIP
20 mg/kg q24h – Ocular FIP
24 mg/kg q24h – Neurological FIP
30 mg/kg q24h – Neurological relapse
When you buy tablets yourself, pay extra attention to find out the information about whether the indicated content of the active substance in the tablet is real, or so-called. equivalent.
Note: Given that there is a reasonable assumption of an absorption limit of GS441524 in the digestive tract, it is recommended for dosages in equivalent 10mg/kg or more when taken orally, divide the dose into 2x a day.
In connection with the treatment of Covid-19, an antiviral drug called Molnupiravir has appeared on the market, which is just a more understandable name for the substance labeled EIDD-2801. Unlike GS-441524, this antiviral drug is used exclusively in oral form. Although its bioavailability (absorption ability) in the digestive tract is similar to that of GS441524, i.e. around 50%, due to the absence of an injectable form, no "equivalent" content of the active substance is used in the recommended dosage by manufacturers and practically all of them state its real content. Thus, no conversion to 50% content is used. A 40mg tablet is simply 40mg, and this must also be taken into account when calculating the dose based on the recommended dosage. And there is one more very important thing... The pharmacokinetics of Molnupiravir is different from that of GS, and therefore Molnupiravir must be administered 2 times a day.
Recommended approximate dosage of EIDD-2801 tablets at 1kg / 12h:
6 mg/kg q12h – Moist FIP
8 mg/kg q12h – Dry FIP
10 mg/kg q12h – Ocular FIP
12 mg/kg q12h – Neurological FIP
15 mg/kg q12h – Neurological relapse
Although at first glance this dosage may seem the same as that of GS, do not forget the essential difference. This is a dosage of 12 hours (as opposed to 24 hours for GS441524).
Given that no official clinical trial has yet been conducted for the use of Molnupiravir in the treatment of FIP (one is currently underway at UC Davis), its use is recommended only in cases of apparent resistance to GS441524, thus Molnupiravir will find application mainly in severe neurological relapses. Keep in mind that the side effects of Molnupiravir are not yet accurately mapped and one of the most feared is the potential mutagenic effect leading to cancer. There is no need to panic, but it is necessary to realize that in the current state of knowledge it is better to use Molnupiravir only in cases where it is really necessary. Time will tell if the possible side effects are a real threat or will never be confirmed.
An interesting paradox occurred in connection with the drugs GS441524 and Molnupiravir (EIDD-2801).
Efficacy and safety of GS441524 in the treatment of FIP was indeed confirmed clinical study, but due to the licensing policy of the patent owner (Gilead company) there is no legal the source of medicines and practically all production is concentrated in China.
On the other hand, the efficacy and safety of Molnupiravir in the treatment of FIP has not yet been confirmed no official clinical study, it exists but is legally available a form of medicine primarily intended for the treatment of Covid-19. In the Czech Republic/SR, it is distributed under the name Lagevrio in packs of 40 capsules, each containing 200 mg of the active ingredient, which is too much. Therefore, for use in cats, the drugs must be decapsulated. Of course, EIDD-2801 is already produced by several Chinese companies that also produce GS441524. Since the drug is not officially intended for the treatment of FIP, it is used off-label.
You are all familiar with the standard treatment for FIP in Australia which uses remdesivir (IV or SCI), GS-441524 (tablets) and mefloquine. These three drugs represent the basic equipment for feline veterinarians in Australia, although the specific details and treatment regimens vary from cat to cat according to their clinical signs and the preferences of the attending physician and the financial resources of the owner. Remdesivir has the advantage of being suitable for both intravenous and subcutaneous treatment, which may be useful in some cases of advanced disease or in cases where the abdominal disease is so extensive that there is concern about how much GS-441524 will be absorbed. I suppose no one uses the polyprenyl immunostimulant anymore despite recent work by the Edinburgh group showing some effectiveness.1
Figure 1: Hong Kong British Shorthair cat with moist (effusive) FIP. Photos courtesy of Chris Simpson.
In fact, some doctors and clients prefer to skip remdesivir altogether and go straight to GS-441524 tablets, which are less expensive, forgoing the need for high-cost hospitalization for several days of intensive treatment. The optimal timing of parenteral administration of remdesivir before switching to GS-441524 tablets is debated. We initially recommended two weeks of parenteral treatment, but for example colleagues at the Royal Veterinary College give remdesivir intravenously for 4-5 days and then switch to oral GS-441524.
Mefloquine is a useful drug that can be used in combination with GS-441524, or it can be given when owners can no longer afford the high cost of treatment, at a time when the cat is doing well but is probably not yet cured. There is some debate about the best dosing regimen for this repurposed drug. The original work suggested that ¼ tablet of Larium (62.5 mg) given twice weekly was adequate, while I prefer 20 to 25 mg per cat once daily. I often start this dose in cats near the end of GS-441524 treatment, and I give mefloquine for several months to give the cat’s immune system a little more time to “clear out” any FIP virus that is hiding in the mononuclear phagocytic cells.
Figure 2: High protein fluid from the abdominal cavity of the cat in Figure 1.
I have found that treatment regimens based on these drugs usually result in successful treatment of kittens and cats with FIP, although individual cases can be very challenging.
In my opinion, the biggest obstacle to successful treatment is the very high cost of treatment. Another problem is the requirement of 84 days of treatment to completely eliminate the virus.
The drugs themselves are very expensive, especially in adult cats or patients with CNS disease (which require higher mg/kg doses for drugs to penetrate the CNS), and this includes not only the very high cost of the drugs, but also the cost of initial stabilization and ongoing consultations for monitoring. As a result, treatment is financially unaffordable for many owners, often from the outset, and if resistance to the FIP virus develops during treatment, the requirement for very high doses, often over a long period of time, makes treatment difficult for even the most dedicated owner.
The owners tried to circumvent the high cost of treatment by using the black market drug GS-441524, which is commonly available from many suppliers. Although it is not legal, owners and especially cat breeders have obtained it in large quantities and many cats have been saved by these drugs.2 The problem is that we are not sure of the actual doses or the quality or the product that is given in different colored tablets, and our testing has shown that the dose, even if indicated on the package, may be higher or lower than the value indicated by the manufacturer. In addition, we cannot assess the differences between individual batches of black market drugs. Therefore, most Australian vets advise clients to use legal products provided by BOVA Australia and the supply chain is reliable and regular quality control ensures that each tablet contains 50mg of GS-4415624 as stated.
Figure 3: X-ray of the cat from Figure 1 with wet FIP.
The COVID pandemic has led to tremendous research into the prevention and treatment of coronavirus disease, and two oral products for the oral treatment of human patients infected with SARS-CoV2, namely molnupiravir and paxlovid, are now commonly available in Australia and elsewhere.3 Niels Pedersen provided the SOC FIP on his website a summary of the history of molnupivirus that I have attached to this monograph. The key part is cut and pasted below (with some editing):
As expected, molnupiravir was recently tested in cats with FIP by at least one Chinese vendor of GS-441524, and preliminary results were reported on the FIP Warriors CZ/SK website. The field study consisted of 286 cats with various forms of naturally occurring FIP seen at companion animal clinics in the US, UK, Italy, Germany, France, Japan, Romania, Turkey and China. There were no deaths among the 286 cats that participated in the tests, including seven cats with ocular (n=2) and neurological (n=5) FIP. Twenty-eight of these cats were cured after 4-6 weeks of treatment and 258 after 8 weeks. All treated cats remained healthy after 3-5 months, which is the period during which cats that were not successfully treated would be expected to relapse.
These data provide compelling evidence for the safety and efficacy of molnupiravir for cats with various forms of FIP. However, we hope that this field study will be written up in manuscript form, submitted for peer review and published. Nevertheless, it is now marketed to owners of cats with FIP. At least one other major marketer of GS-441524 is also interested in using molnupiravir to treat FIP, indicating demand for additional antiviral treatment in cats with FIP.
The safe and effective dosing of molnupiravir in cats with FIP has not been published. However, at least one vendor from China provided some pharmacokinetic and field test data for molnuparivir in cats with naturally occurring FIP in their promotional leaflet for a product called Hero-2801. In 28/286 cases, they received this drug at a dose of 30-40 mg/kg every 24 hours, ie the equivalent of 15-20 mg/kg every 12 hours. For comparison, the dose for humans is 800 mg every 12 hours or about 10 mg/kg per day.
Figure 4: Data provided on “Hero 2018” by FIP Warriors CZ/SK – EIDD-2801 (Molnupiravir). https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/
Dosage recommendations seem to vary. It was originally proposed:
FIP: 25mg/kg q24h
Ocular FIP: 37.5 mg/kg q24h
Neurological FIP: 50 mg/kg q24h
The duration of treatment is 5-10 weeks, depending on the severity of the disease and the specific cat.
Later, this proposal was modified based on input from Niels Pedersen and the UC Davis group:
FIP: approximately 5-7 mg/kg q12h for 84 days.
Ocular FIP: 8-10 mg/kg q12h for 84 days.
Neurological FIP: 10-15 mg/kg q12h for 84 days.
These recommendations are based on assumptions based on published information and more field experience with molnupiravir is needed. Sam Evans has just presented some data on the use of molnupiravir for salvage therapy at the ISCAID conference in Glasgow. An active clinical trial involving Brian Murphy and Krystal Regan is underway at the University of California, Davis, to determine the optimal dosage and dosing interval for molnupiravir, beginning in July 2022.
It is questionable whether molnupiravir will prove safer and more effective than GS-441524 in the treatment of FIP, but a third antiviral could prove extremely useful in preventing resistance to GS-441524 (as a cocktail of antivirals with different resistance profiles) or in treating cats that they no longer respond well to GS-441524. The big unknown is whether molnupiravir will be free of long-term side effects.
As the dosages given in the trials seem to be somewhat questionable, I used 10mg/kg twice daily, but note that test cats are claimed to have received 100mg/kg once daily with no detectable adverse effects (see Figure 4) .
Key fact: I have been using molnupiravir in selected patients for about 2 months at a dose of 10 mg/kg twice a day. It may be prudent to increase this dose to 15 mg/kg twice daily, particularly in CNS disease. Higher doses seem likely to be safe and possibly more effective, but I'm reluctant to recommend them until we get more long-term data.
Finally, and really on a side note, paxlovid is a combination of two drugs given at the same time, with one used to inhibit the metabolism of the other; I can find no precedent for its use in cats, which is a shame because in humans it is the more effective of the two oral drugs available for COVID. It costs about the same in Australia as molnupiravir, but is comparably more expensive than molnupiravir when purchased from websites in India. It could prove to be a very useful drug for treating FIP if it is proven safe. In humans, one of the problematic side effects is a foul taste in the mouth, so-called “paxlovid mouth”, which could prove disastrous if it were to occur in cats, as they tend to foam at the mouth.
So what is the place of molnupiravir in the therapy of kittens and cats with FIP? How to get it? How much does it cost?
Anyone can buy molnupiravir for personal use or for use in cats by obtaining a prescription and presenting it at a pharmacy. The price is approximately $1,146.39 (https://www.pbs.gov.au/medicine/item/12910L) subject to pharmacy surcharge. The trade name is Lagevrio (Merck Sharp & Dohme) and the box contains 40×200 mg capsules. The drug was provisionally approved by the TGA in February 2022 for the treatment of COVID-19 in adults who do not require oxygen and are at risk of progression to severe COVID-19.
To treat a 4 kg cat at 10-15 mg/kg bid, you need 80 mg to 120 mg daily for 84 days or 6,720 to 10,080 mg. A box of 40x200 mg capsules is 8,000 mg, so if you factor in the preparation fee for a suitable dose for a cat - the high dose treatment costs about $1100-$2200, which is quite a bit cheaper than GS-441524 or remdesivir. So now we have an alternative treatment to the one we are currently using. What is the evidence? Are pharmacokinetics well known in cats? The answer to both is - we don't know for sure because the evidence hasn't been peer-reviewed, but compelling unpublished anecdotal information suggests it's an effective therapy. And we'll probably have good PK info from the Davis group within a year.
And now it gets a little more complicated! Australia has a system that allows people to import medicines from overseas for their own personal use and that of their family members. The reason is that human patients who are prescribed expensive unregistered medicines, and therefore medicines not covered by the PBS, have to find their own way of getting these medicines. It is not known how many Australians import medicines, but it is legal under the personal import scheme. Perhaps the best example is the “FixHepC Buyers Club” (https://fixhepc.com/), founded by Australian infectious disease doctors and general practitioners Drs John and James Freeman.5 Before hepatitis C drugs were subsidized by the PBS, thousands of Australians used this buyers' club to import affordable hepatitis C drugs at 1-2 % of the retail price. The initiative was supported by the Australian Society for HIV, Viral Hepatitis and Sexual Health Medicine, and many Australian doctors directed patients to buy their medication this way.
"They each paid $1,000 to $2,000 to get better, instead of the $84,000 that Gilead Sciences charged in America. It's still expensive, but at least it's affordable for many."
However, it comes with some risk. The online market for medicines is poorly regulated, operating across jurisdictions and substandard products are common. Some estimates suggest that up to 25% of medicines in circulation outside high-income countries are substandard. The biggest risk is insufficient quantities of the active substance, which can lead to unintentional undertreatment. This is a difficult area for doctors to navigate, both clinically and medico-legally. It is unclear how far a doctor’s duty of care extends. The current code of conduct states that good medical practice includes “upholding the patient’s right to access the necessary level of healthcare and, wherever possible, assisting them to do so.” There is no reason to believe that this would not also include helping patients to import medicines they would otherwise be unable to afford, if it is clearly in their best interest to do so.
My own opinion is that this is the same situation for small animal vets involved in the treatment of cats with FIP, and the vet oath taken by recent graduates would support this claim.
So how can a client order molnupiravir to treat their cat with FIP?
Figure 5; Screenshot of correspondence with the manufacturers of Molcovir 200 mg
Go to the internet and find the URL of the website called IndiaMART https://www.indiamart.com/ and search for Molcovir 200mg - currently the URL is: https://m.indiamart.com/isearch.php?s=Molcovir +200mg&prdsrc=1&countryiso=AU&qu-cx=1&stype=attr=1
They will take your information and ask what medicine you are interested in. They will then send your inquiry to several pharmacies and ask you for quotes. The manufacturers we have the most experience with are Dolphin pharmaceuticals and Mediseller, one of which accepts payment via PayPal instead of using your credit card. They will advise you that customs is your own business, but they will do their best to help you label the medication so that it is clear that it is not an illegal drug. You can't buy anything until the quote comes back to you. Figure 5 shows a screenshot of the correspondence with the company. Once you accept the quote, they will then arrange payment and then shipping. Currently, a five-pack purchase costs US$30 (AU$42) per pack plus US$65 shipping. Treating a 4kg cat with FIP CNS at 10-15mg/kg bid for 84 days is likely to be in the range of AUD$100-150. The cost of treating the same cat with remdesivir/GS-441524 is $6,550 when drug costs alone are considered.
So the cost of treating a cat with molnupiravir from India under the personal importation scheme will be about 2 % of the cost of conventional GS-441524 treatment. This means that no cat has to be euthanized due to the high cost of treatment –
Figure 6; Generic molnupiravir (Molcovir 200 mg capsules) purchased from IndiaMART and imported to Australia after customs clearance
The practical question is how to obtain molnupiravir in time. When purchased from this website, it takes approximately 3 weeks for the drug to reach Australia and clear customs. One option would therefore be to start treatment with remdesivir and/or GS-441524 and switch to molnupiravir as soon as the drug arrives. An alternative is to set up a “buyers’ club”, perhaps with the support of the Australian and New Zealand College of Veterinary Science Pharmacology chapter, to be the source of molnupiravir until the client can arrange to import their own supplies. Another option would be for a compounding pharmacy to import the drug from a reliable manufacturer and adapt it to a size suitable for cats and kittens, perhaps as a 60 mg metered tablet that can be split in half.
What is the best way to treat a cat with FIP in 2022 in Australia?
This question is not as simple as it might seem. Remdesivir and GS-441524 have had much success as a treatment for FIP in kittens and cats, and we are also comfortable with low-dose mefloquine as an add-on to consolidate treatment. However, most of us who have assisted in the treatment of cats know of cases where the FIP virus has developed acquired mutational resistance during treatment. This can often be worked around by increasing the doses of GS0-441524 administered, but many owners simply cannot afford this procedure.
Thus, the routine use of combination therapy of FIP cases using GS-441524 and molnupiravir can be recommended, and it is indeed possible that the combination therapy could be more effective and faster because it attacks two different targets in the FIP virus, and this could potentially lead to a shorter duration of treatment. The idea of 84-day therapy comes from the seminal work of Neil Pedersen and perhaps the assumption that the lifespan of macrophages in tissues is about 84 days, so to completely eliminate all the intracellular virus that is hiding in the mononuclear phagocyte system, we need to treat for longer than 84 days of lifespan macrophage.
However, for many clients, the huge cost of treatment is an insurmountable problem, and for many, and I dare say most clients, the ability to treat their kitten or cat for $200 (drug costs) will be the most important argument.
What is the disadvantage of molnupivir? The big unknown is whether molnupiravir will not have long-term toxic effects, since the active substance, N4-hydroxycytidine, is an extremely potent mutagen and the treatment time for FIP is much longer than the 5 days recommended for the treatment of Covid-19 in human patients. The probability of side effects is therefore theoretically higher. To me, that's a completely theoretical risk, but it's something we have to monitor in the patients we treat, being aware of the possibility of later cancer in some cases.
References
1. Černá, P.; Ayoob, A.; Baylor, C.; Champagne, E.; Hazanow, S.; Heidel, RE; Wirth, K.; Legendre, AM; Gunn-Moore, DA Retrospective Survival Analysis of Cats with Feline Infectious Peritonitis Treated with Polyprenyl Immunostimulant That Survived over 365 Days. Pathogens2022, 11, 881. https://doi.org/10.3390/pathogens11080881
2. Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S. Unlicensed GS-441524-Like Antiviral Therapy Can Be Effective for At-Home Treatment of Feline Infectious Peritonitis. Animals2021, 11,2257. https://doi.org/10.3390/ani11082257
3. Atmar RL, Finch N. New Perspectives on Antimicrobial Agents: Molnupiravir and Nirmatrelvir/Ritonavir for Treatment of COVID-19. Antimicrob Agents Chemother. 2022 Aug 16;66(8):e0240421. doi: 10.1128/aac.02404-21. Epub 2022 Jul 12. PMID: 35862759; PMCID: PMC9380556.
4. https://ccah.vetmed.ucdavis.edu › files › inline-files (this is a fantastic review of this subject, although some of the arithmetic is wrong. Highly recommended for people who are interested in drug development and action.)
This article discusses the development of knowledge about feline infectious peritonitis (FIP) from its recognition in 1963 to the present and has been prepared to inform veterinarians, cat rescuers and carers, shelter staff and cat lovers. The causative agent of the feline coronavirus and its relationship to the ubiquitous and minimally pathogenic feline intestinal coronavirus, epizootology, pathogenesis, pathology, clinical signs and diagnostics are briefly mentioned. The main emphasis is placed on the risk factors influencing the incidence of FIP and the role of modern antivirals in successful treatment.
Introduction
Figure 1. Photo of the author and Dr. Jean Holzworthová (1915-2007) from 1991. Dr. Holzworth was the best feline veterinarian the author knew and was responsible for the first report of FIP as a specific disease. She spent her entire career at Angell Memorial Animal Hospital in Boston.
Feline infectious peritonitis (FIP) was described as a specific disease in 1963 by veterinarians at Angell Memorial Animal Hospital in Boston (Holzworth 1963) (Fig. 1). Pathology records from this institution and Ohio State University failed to identify earlier cases (Wolfe and Griesemer 1966), although identical cases were soon recognized worldwide. The initial pathological descriptions were of diffuse inflammation of the tissues lining the abdominal cavity and abdominal organs with extensive effusion of inflammatory fluid, after which the disease was eventually named (Wolfe and Griesemer 1966, 1971) (Figs. 2, 3). A second and less common clinical form of FIP, which presents with less diffuse and more widespread granulomatous lesions involving organ parenchyma, was first described in 1972 (Montali and Strandberg 1972) (Figs. 3,4). The presence of inflammatory effusions in the body cavity in the common form and the absence of effusions in the less common form led to the names wet (effusion, non-parenchymatous) and dry (non-effusion, parenchymatous) FIP.
The prevalence of FIP appears to have increased during the panzootic disease caused by feline leukemia virus (FeLV) in the 1960s–1980s, when many cases of FIP were found to be associated with FeLV (Cotter et al., 1973; Pedersen 1976a). The subsequent management of FeLV infection in domestic cats through rapid testing and vaccination resulted in an increase in the number of FIP cases. However, recent interest in breeding/rescue along with effective treatment has led to increased awareness of the disease and its diagnosis.
Figure 2. Gross necroptic appearance of the abdominal cavity of a cat with acute onset wet FIP. The abdomen is filled with several hundred ml of yellow viscous fluid, the omentum is reddened, edematous and contracted, and fibrin deposits (arrows) are visible on the surface of the spleen and the edges of the liver. A fiber of fibrin can be seen on the spleen
Figure 3. Appearance of an open abdomen at autopsy of a cat that died of a chronic form of effusive FIP. The abdomen is filled with a viscous, yellow-colored exudate, and the omentum is thickened and contracted. The main lesions are in the liver with numerous plaque-like structures (pyogranulomas) on the cover. More circumscribed lesions (granulomas), also oriented on the serous surface, look more fleshy and are elevated above the surface. These lesions also involve the underlying liver parenchyma and are more typical of dry FIP. This is an example of a case of FIP that transitions between the wet and dry forms (arrow).
Figure 4A – Gross section of kidneys of two cats with dry form of FIP. The lesions are superficial and extend into the underlying parenchyma.
Figure 4B - lesions of the dry form of FIP in organs such as the kidneys, cecum, colon and intestinal lymph nodes (Fig. 5) were grossly confused with renal lymphoma.
Figure 5. Gross enlargement of ileo-cecal-colic lymph nodes in a cat with dry FIP.
Etiological factor
The first attempts did not allow identifying the causative agent of FIP, but confirmed its infectious nature (Wolfe and Griesemer 1966). A viral etiology was established in 1968 using ultrafiltrates of infectious material (Zook et al., 1968). The causative virus was subsequently identified as a coronavirus (Ward 1970), which is closely related to enteric coronaviruses of dogs and pigs (Pedersen et al., 1978).
Confusion arose when feline enteric coronavirus (FECV) was isolated from the feces of healthy cats and proved to be indistinguishable from feline infectious peritonitis virus (FIPV) (Pedersen et al., 1981). Unlike FIPV, which readily induced FIP in laboratory cats, experimental infections with FECV were largely asymptomatic. The relationship between the two viruses became clear when FIPVs were found to be FECV mutants that arise in the body of every cat with FIP (Vennema et al., 1995; Poland et al., 1996).
FECV is ubiquitous in feline populations worldwide and is first shed in faeces from approximately 9–10 weeks of age, coinciding with the loss of maternal immunity (Pedersen et al., 2008 ;). The infection takes place via the faecal-oral route and targets the intestinal epithelium, and the primary signs of enteritis are mild or inconspicuous (Pedersen et al., 2008; Vogel et al., 2010). Subsequent faecal excretion occurs from the colon and usually stops after several weeks or months (Herrewegh et al., 1997; Pedersen et al., 2008; Vogel et al., 2010). Immunity is short-lived and repeated infections are common (Pedersen et al., 2008; Pearson et al., 2016). Over time, stronger immunity eventually develops and cats older than 3 years are less likely to shed the infection in their faeces (Addie et al., 2003). FECV is constantly subject to genetic drift into locally and regionally identifiable clades (Herrewegh et al., 1997; Pedersen et al., 2009).
FECV and FIPV are classified as biotypes of the feline coronavirus (FCoV) subspecies. The genomes of FECV and FIPV biotypes are related at >98 %, but with unique host cell tropism and pathogenicity (Chang et al., 2012; Pedersen et al., 2009). FECVs infect the mature intestinal epithelium, whereas FIPVs lose intestinal tropism and acquire the ability to replicate in monocytes/macrophages. The published names FECV or FIPV will be used here when discussing aspects of the disease specific to each biotype, while the term FCoV will be used when discussing features common to both biotypes.
Three types of mutations are involved in the biotype change of FECV to FIPV. The first type, which is unique to each cat with FIP (Poland et al., 1996), consists of an accumulation of missense and nonsense mutations in the c-terminus of the auxiliary 3c gene, often resulting in truncated 3c gene products (Pedersen et al., 2012 ; Vennema et al., 1995). The second type of mutation consists of two specific single nucleotide polymorphisms in the fusion peptide of the S gene, one or the other form being common to >95 % FIPV and absent in FECV (Chang et al., 2012). A third type of mutation, unique to each FIPV isolate and not found in FECV, occurs in and around the furin cleavage motif between the receptor binding domain (S1) and the fusion domain (S2) of the spike gene (S) (Licitra et al., 2013). These mutations have different effects on furin cleavage activity. Together and in an as yet undetermined manner, they are responsible for the shift of the tropism of the host cell from the enterocyte to the macrophage and for the profound change in the form of the disease.
FCoV, and therefore FECV and FIPV, exist in two serotypes identified by antibodies against the viral neutralizing epitope on the S gene (Herrewegh et al., 1998; Terada et al., 2014). Serotype I FCoVs are identified in cat sera and are prevalent in most countries. Serotype II FCoVs result from recombination with the S part of the canine coronavirus gene (Herrewegh et al., 1998; Terada et al., 2014) and are identified by canine coronavirus antibodies. Serotype II FIPVs are easily cultured in tissue culture, whereas serotype I FIPVs are difficult to adapt to growth in vitro. Serotype I and II FECVs were not grown in conventional cell cultures (Tekes et al., 2020).
FIPVs are found exclusively in activated monocytes and macrophages in affected tissues and effusions and are not secreted into the environment. Therefore, cat-to-cat (horizontal) transmission of FIPV is not the main mode of spread. Rather, FIP follows the pattern of an underlying enzootic FECV infection, with sporadic cases and occasional small outbreaks of disease (Foley et al., 1997). These clusters of cases can be mistaken for epizootics. The only report of an epizootic occurrence of FIP was associated with a single serotype II virus that appeared to develop in a shelter housing both dogs and cats (Wang et al., 2013). Horizontal transmission in this case followed an epizootic rather than an enzootic disease model, with infection spreading rapidly to cats of all ages and in close contact with the index case (Wang et al., 2013).
The low incidence of FIP cases in the population suggests that FIPV mutations arise infrequently. However, studies involving FECV infection in immunocompromised cats infected with FIV and FeLV suggest that FIP mutants may be common but only cause disease under certain circumstances. Nineteen cats infected with feline immunodeficiency virus (FIV) for 6 years and a control group of 20 littermates not infected with FIV were orally challenged with FECV (Poland et al., 1996). Cats in both groups remained asymptomatic for two months when two cats in the FIV-infected group developed FIP. In a second study, 26 young cats with enzootic FECV infection from a breeding colony with no history of FIP were contact-exposed to FeLV carriers (Pedersen et al., 1977). Two kittens in the group subsequently developed FIP 2–10 weeks after becoming FeLV viremic. The question remains, how long can FIPV viruses survive in the body before they are eliminated? According to one of the theories, they persist in the body for a certain time and become pathological only if immunity against them is impaired (Healey et al., 2022). This theory is supported by the way immunity to FeLV develops. Most cats resist FeLV by kitten age and develop robust and permanent immunity, but this occurs within a few weeks, during which the virus persists in a subclinical or latent state (Pedersen et al., 1982; Rojko et al., 1982). . Methylprednisolone given during this period, but not after, will abolish developing immunity and lead to a state of persistent viremia.
Epizootology
Epizootiology is the study of the occurrence, spread and possible control of animal diseases and the influence of environmental, host and agent factors. FIP is considered one of the most important infectious causes of death in cats, although there are no precise data on prevalence. It is estimated that 0.3–1.4 % deaths of cats presented to veterinary institutions are related to FIP (Rohrbach et al., 2001; Pesteanu-Somogyi et al., 2006; Riemer et al., 2016) and in some shelters and breeding stations up to 3.6–7.8 % (Cave et al., 2002). FIP is also described as an environmental disease with a higher incidence of multiple cats. Three-quarters of the FIP cases in the currently ongoing treatment study came from the field through foster carers/rescues and cat shelters, 14 % from kennels, and only 11 % from households.1
Studies based on cases observed in academic institutions have demonstrated the influence of age and gender on the incidence of FIP (Rohrbach et al., 2001; Pesteanu-Somogyi et al., 2006; Pedersen 1976a; Worthing et al., 2012; Riemer et al., 2016) . Three-quarters of the cases in these cohorts occurred in cats younger than 3 years of age, and few cases occurred after 7 years of age. This was also confirmed by a current and ongoing field study from the Czech Republic and Slovakia, in which it was found that more than 80 % cases of FIP occurred in cats under 3 years of age and only 5 % in cats older than 7 years (Fig. 6) .1 Earlier institutional studies differed on the effect of sex, but indications were that male cats were slightly more susceptible to FIP than female cats. This was also confirmed by current data from the field, which show a ratio of males to females of 1.3:1.1. It is unclear whether castration affects the incidence of FIP, with some reports suggesting that it may increase susceptibility (Riemer et al., 2016), while others do not report such a clear effect.1
Figure 6. Age of more than 607 cats from the Czech Republic and Slovakia at the time of diagnosis and treatment of FIP.1 Thirty percent of infections were in cats six months of age or younger, 50 % at one year of age, and 85 % at three years of age or younger.
Other environmental and viral risk factors have been implicated in the increased incidence of FIP, but their significance requires knowledge of disease occurrence in their absence. A possible baseline may have been provided by a study of enzootic FECV infection, which had been unrecognized for many years in a well-managed specific pathogen-free breeding colony (Hickman et al., 1995). This colony was kept in strict quarantine free of other infections and the standard of nutrition and husbandry was high. This colony produced hundreds of kittens each year before the first case of FIP was diagnosed. Such observations suggest that FIP may be a rare phenomenon in the absence of risk factors.
The importance of moving to a new home as a risk factor for FIP is only now being appreciated. Breeders, many of whom have not experienced any cases of FIP in their litters, are most concerned about the announcement that one of their kittens has developed FIP shortly after going to a new home. A recent study found that more than half of cats with FIP had experienced a change in environment, shelter or capture in the weeks before the illness.1 Cats are known to hide external signs of stress even when they are suffering from serious internal ill effects. Even simple procedures such as changing the cage will suppress immunity and reactivate latent herpes virus shedding and disease symptoms in cats (Gaskell and Povey, 1977). Stressful situations, even those that appear to be minor, can cause a decrease in lymphocyte levels and “sick behavior” (Stella et al., 2013).
Differences in the genetic make-up of enzootic FCoV strains may also contribute to the prevalence of FIP in the population. Serotype II FIPVs are thought to be more virulent than serotype I and more likely to be transmitted from cat to cat (Lin et al., 2009; Wang et al., 2013). It is also possible that certain FECV clades are more susceptible to mutation to FIPV, which should be studied. The author also observed a disproportionately high proportion of cats with neurologic FIP in some regions, suggesting that genetic determinants in certain FCoV strains may be more neurotropic.
Immunodeficiencies associated with retroviruses are associated with susceptibility to FIP. Up to half of FIP cases during the peak of FeLV panzootic disease were persistently infected with FeLV (Cotter et al., 1973; Pedersen 1976a; Hardy 1981). FeLV infection causes suppression of T-cell immunity, which may inhibit the protective immune response to FIP. The importance of FeLV infection for the incidence of FIP has declined significantly since the 1980s, when carrier elimination and vaccination pushed FeLV back into the wild, where exposures are less severe and immunity is the usual outcome. Chronic feline immunodeficiency virus (FIV) infection has also been shown to be a risk factor for FIP in FECV-infected cats under experimental conditions (Poland et al., 1996). In one recent field study, FeLV infection was recognized in 2 % and FIV in 1 % cats treated for FIP.1
The incidence of FIP in purebred cats is reported to be higher than in random breeding cats, with some breeds appearing to be more susceptible than others (Pesteanu-Somogyi et al., 2006; Worthing et al., Genetic predisposition to FIP has been investigated in several Persian cat breeds and is estimated to account for half the risk of the disease (Foley et al., 1997). Some breeds, such as the Birman, are more susceptible to developing dry than wet FIP (Golovko et al., 2013). Attempts to identify specific genes associated with susceptibility for FIP in Burmese cats included several immune-related genes, but none reached the desired significance (Golovko et al., 2013).The largest study of genetic susceptibility to FIP showed that it is extremely polymorphic and reported consanguinity as a major risk factor. breeding (Pedersen et al., 2016).Specific polymorphisms in several genes have also been associated with high levels of FECV shedding among several breeding cat breeds (Bubeniko and et al., 2020).
In females, FIP, usually the wet form, may develop during pregnancy or in the perinatal period. This phenomenon resembles the suppression of immunity in pregnant women and the predisposition to certain infections (Mor and Cardenas 2010). It is not clear whether subclinical FIP is activated by pregnancy or by increased susceptibility to new infection. Maternal infection early in pregnancy results in fetal death and resorption, while later infections often result in abortion (Fig. 7). Kittens can be born healthy, but develop disease in the perinatal period and die. Some babies are born uninfected thanks to the effectiveness of the placental barrier between mother and fetus or thanks to the help of antiviral treatment (Fig. 8).
Figure 7. Aborted kittens from a dam that developed wet FIP late in pregnancy. Miscarriage was the first symptom of FIP, quickly followed by the classic symptoms of abdominal wet FIP. The mother was successfully cured of FIP with the antiviral GS-441524.
Figure 8. This mother developed symptoms of wet abdominal FIP 3 weeks after the onset of pregnancy and was successfully treated with GS-441524. Subsequently, she gave birth to a litter of four kittens by caesarean section, one of which died and three survived and grew up healthy. Treatment was given during the remaining 6 weeks of gestation and continued for 6 weeks during which the kittens were successfully nursed. GS-441524 had no apparent side effects on the mother or the kittens.
A possible increase in the number of cases of FIP was observed in cats older than 10 years in studies conducted 50 years ago (Pedersen 1976a). Slightly more than 3 % cases of FIP in a recent study occurred in cats 10 years of age and older and 1.5 % in cats 12 years of age and older (Fig. 6).1 The occurrence of FIP in the elderly often involves two different scenarios. The first scenario also involves exposure to FECV faecal excretion, but in a unique way. It is common for old cats to mate as kittens and live together in relative isolation unexposed to FECV for many years. One cat in the pair dies, is left alone, and a much younger companion obtained from a rescue organization, shelter, or kennel is brought into the household that has a high probability of excreting FECV. Older cats are also susceptible to the same FIP risk factors as younger cats, as well as other factors associated with aging. The first of these is the impact of aging on the immune system, with the most consequential being the deterioration of cellular immune function (Day 2010). Other risk factors associated with old cats include the debilitating and potentially immunosuppressive effects of diseases such as cancer and chronic diseases of the kidneys, liver, oral cavity and intestines. Some diseases in old cats can be mistaken for FIP or complicate the treatment of FIP if they are present at the same time.
Other risk factors that need further investigation include loss of maternal systemic immunity by separation at birth, early weaning and loss of lactogenic immunity, malnutrition, common kitten infectious diseases, early neutering, vaccination, congenital heart defects, and even a shelter fire (Drechsler et al.), 2011; Healey et al., 2022; Pedersen 2009, Pedersen et al. 2019).1 However, the most important positive risk factor remains the presence of FECV in the population (Addie et al., 1995). The prevalence of FIP in several Persian cat breeds was also related in one study to the proportion of cats that shed FECV at a given time and to the proportion of these cats that are chronic shedders (Foley et al., 1997). The importance of exposure to FECV supports the need to find ways to either prevent infection or reduce its severity. One of the first steps is a better understanding of FECV immunity (Pearson et al., 2019).
Pathogenesis
The first interface between FECV and the immune system is the lymphatic tissues of the intestine (Malbon et al., 2019, 2020). Although the downstream events leading to FIP are not fully understood, it is possible to speculate based on what is already known about FECV and FIPV infections, other macrophage-tropic infections, and viral immunity in general. During intestinal infection, FECV particles and proteins reach the local lymphatic tissues and are processed by phagocytic cells first into peptides and finally into amino acids. Some of these peptides will be recognized as foreign when arrayed on the cell surface, triggering innate (innate or non-specific) and adaptive (acquired or specific) immune responses (Pearson et al., 2016). FECVs also mutate to FIPV at the same time and in the same cell type. Some of these mutations will allow the virus to replicate in these or closely related cells of a specific monocyte/macrophage lineage.
The host cell for FIPV appears to be a specific class of activated monocytes found around venules on the surface of intestinal and thoracic organs, mesentery, omentum, uveal tract, meninges, choroid and ependyma of the brain and spinal cord, and freely in effusions. These cells belong to the activated (M1) class (Watanabe et al., 2018) and resemble a subpopulation of small peritoneal macrophages described in mice (Cassado et al., 2015). This type of cell arises from circulating bone marrow-derived monocytes that are rapidly mobilized from the blood in response to infectious or inflammatory stimuli. A similar-looking population of activated monocytes has been described around blood vessels in the retina affected by FIP (Ziolkowska et al., 2017). These cells stained for calprotectin, indicating their blood origin. Although FIPV infection occurs initially in smaller activated monocytes, viral replication is most intense in large, vacuolated, terminally differentiated macrophages (Watanabe et al., 2018). The virus released from these cells rapidly infects activated monocytes produced in the bone marrow and drawn to the site from the bloodstream.
The cellular receptor used by FECVs to infect intestinal epithelial cells has not yet been determined. The cellular receptor that FIPVs use to infect activated monocytes is also unknown. RNAs for conventional coronavirus receptors such as aminopeptidase N (APN), angiotensin converting enzyme 2 (ACE2) and CD209L (L-SIGN) were not upregulated in infected peritoneal cells of cats with experimental FIP, and CD209 (DC-SIGN) was significantly underexpressed (Watanabe et al., 2018). An alternative route of infection of activated monocytes may involve immune complexation of the virus and entry into cells by phagocytosis (Dewerchin et al., 2008, 2014; Van Hamme et al., 2008). Activated monocytes in lesions stain strongly positive for FIPV antigen, IgG and complement (Pedersen, 2009) and mRNA for FcγRIIIA (CD16A/ADCC receptor) is markedly increased in infected cells (Watanabe et al., 2018), supporting infection through immune complexation and alternative receptors related to phagocytosis.
Macrophage pathogens are intracellular and elimination of infected cells occurs through lymphocyte-mediated killing. The first line of defense is non-specific lymphocytes, and if they fail, an adaptive immune response to FIPV follows through specific T-lymphocytes. If infected activated monocytes and macrophages fail to be contained and eliminated, they may disseminate locally in the abdominal cavity, possibly from lymph nodes in the lower intestinal region and the site of FECV replication. Spread locally and to distant sites via the bloodstream is by infected monocyte cells (Kipar et al., 2005).
FIP occurs in two basic forms, wet (effusive, nonparenchymatous) (Figures 2 and 3) or dry (noneffusive, parenchymatous) (Figures 4 and 5), with wet FIP accounting for 80 % cases.1 The term “wet” refers to the characteristic effusion of fluid in the abdomen or chest (Wolfe and Griesemer 1966, 1971). Wet FIP lesions are dominated by inflammation resembling immediate- or Arthus-type hypersensitivity (Pedersen and Boyle, 1980), whereas dry FIP lesions resemble delayed-type hypersensitivity reactions (Montali and Strandberg 1972; Pedersen 2009). Wet and dry forms of FIP therefore reflect competing influences of antibody- and cell-mediated immunity and associated cytokine pathways (Malbon et al., 2020, Pedersen 2009). Immunity to FIPV-infected cells, which is the norm, is thought to involve strong cell-mediated responses (Kamal et al. 2019). Dry FIP is thought to occur when cell-mediated immunity is partially effective in suppressing infection, while wet FIP occurs when cell-mediated immunity is ineffective and humoral immune responses predominate.
FIP is considered unique among macrophage infections because it is viral, but the dry form shares many clinical and pathogenic features with feline diseases caused by systemic mycobacterial (Gunn-Moore et al., 2012) and fungal infections (Lloret et al., 2013). . Similarities in pathogenesis also exist between wet FIP and antibody-enhanced viral infections such as dengue fever and dengue hemorrhagic shock syndrome (Pedersen and Boyle 1980; Rothman et al., 1999; Weiss and Scott 1981).
Host responses are thought to solely determine the outcome of FIPV infection and the resulting forms of disease. However, macrophage-tropic pathogens have evolved their own unique defense mechanisms against the host (Leseigneur et al., 2020). One of the mechanisms is the delay of programmed cell death (apoptosis). Delayed apoptosis allows sustained microbial replication and eventual release of more infectious agents, as has also been described in FIPV-infected macrophages (Watanabe et al., 2018). FIPV can also control the recognition and killing of infected activated monocytes by specific or non-specific T-cells. The cell surface targets for T-cells that kill infected cells are likely FIPV proteins (antigens) expressed on major histocompatibility complex class I (MHC-I) receptors. However, surface expression of viral antigens by MHC-I receptors was not detected on FIPV-positive cells collected from FIP tissues or effusions (Cornelissen et al., 2007). DC-Sign has been proposed as a receptor for FIPV (Regan and Whitaker, 2008), but RNA for DC-Sign is markedly underexpressed by infected peritoneal cells, whereas RNA for Fc (MHC-II) receptors is markedly overexpressed and RNA for MHC -I is reduced (Watanabe et al., 2018). This suggests that the normal mode of infection of host cells may be altered by FIPV to favor infection by phagocytosis instead of binding to specific viral receptors on the cell surface, fusion with the cell membrane, and internalization.
Pathology
Detailed descriptions of the gross and microscopic lesions in the wet form of FIP were first described by Wolfe and Griesemer (1966, 1971). The disease is characterized by vasculitis involving venules in the tissues lining the abdominal or thoracic cavity, organ surfaces, and supporting tissues such as the mesentery, omentum, and mediastinum. The inflammatory process leads to effusions in the abdominal or chest cavity up to a volume of one liter or more (Fig. 2, 3). The underlying lesion is a pyogranuloma, which consists of a focal accumulation of activated monocytic cells in various stages of differentiation, interspersed with non-degenerate neutrophils and sparse numbers of lymphocytes. Pyogranulomas are superficially oriented and appear grossly and microscopically as single and coalescent plaques (Fig. 2).
FIPV antigen is immunohistochemically (IHC) observed only in activated monocytes in lesions and effusions (Litster et al., 2013). Large vacuolated terminally differentiated macrophages are particularly rich in virus (Watanabe et al., 2018), reminiscent of the lepromatous form of leprosy (deSousa et al., 2017). Lymph nodes located near the sites of inflammation are hyperplastic and enlarged.
The relationship between dry and wet FIP was first described in 1972 in a report of cases of unknown etiology with similar pathology (Montali and Strandberg 1972). As the authors state, “this pathological syndrome was characterized by granulomatous inflammation in various organs, but mainly affected the kidneys, visceral lymph nodes, lungs, liver, eyes, and leptomeninges.” Tissue extracts from these lesions induced wet FIP in laboratory cats, confirming that wet and dry FIP are caused by the same agent.
The gross and microscopic pathology of dry FIP resembles that of other macrophage-tropic infections such as feline systemic blastomycosis, histoplasmosis, coccidioidomycosis (Lloret et al., 2013), tuberculosis and leprosy (Gunn-Moore et al., 2012). Lesions of dry FIP mainly involve the abdominal organs (Figs. 5, 6) and are rare in the thoracic cavity (Montali and Strandberg 1972; Pedersen 2009). Lesions are less widespread and focal than in wet FIP, with a tendency to extend from the serous surfaces into the parenchyma of the underlying organs (Figs. 5, 6). The target of the host immune response are small aggregates of infected monocytic cells associated with venules, similar to pyogranulomas in wet FIP, but surrounded by dense accumulations of lymphocytes and plasma cells and variable fibrosis. The florid hyperemia, edema, and microhemorrhage associated with wet FIP are mostly absent, therefore significant effusions in the body cavities are absent. The host response to foci of infection gives the lesions a gross tumor-like appearance (Figs. 5, 6). Infected activated monocytes in the central focus of infection are less dense and contain lower levels of virus than in the wet form (Pedersen 2009;), a feature of the tuberculoid form of leprosy (de Sousa et al., 2017). Lesions in some places, for example on the wall of the large intestine, can cause a dense surrounding zone of fibrosis, which resembles classic tuberculosis granulomas. Transitional forms also exist between wet and dry forms in a small number of cases and are mostly recognizable at autopsy (Fig. 3).
Ocular and neurological FIP are classified as forms of dry FIP (Montali and Strandberg 1972). However, pathology in the uveal tract and retina and in the ependyma and meninges of the brain and spinal cord is intermediate between wet and dry FIP (Fankhauser and Fatzer 1977; Peiffer and Wilcock 1991). This can be explained by the effect of the blood-ocular and blood-brain barrier in protecting these areas from systemic immune reactions.
Clinical characteristics of FIP
The five most common symptoms in cats with FIP, regardless of clinical form and frequency of occurrence, are lethargy, loss of appetite, enlarged abdominal lymph nodes, weight loss, fever, and deteriorating coat.1 These symptoms can appear quickly, within a week, or they can exist for many weeks or even months before a diagnosis is made. The course of the disease tends to be more rapid in cats with wet FIP than with dry FIP, and growth retardation is common in young cats, especially those with more chronic disease. 20 % cats with fever as the main symptom are eventually diagnosed with FIP (Spencer et al., 2017).
The wet form of FIP occurs in approximately 80 % cases, more often in younger cats, and tends to be more severe and more rapidly progressive than the dry form. Abdominal effusion (ascites) is four times more common than pleural effusion, with abdominal distension (Fig. 9) and dyspnea being common symptoms. Pyrexia and jaundice are more common symptoms in cats with wet than dry FIP (Tasker, 2018).
Figure 9. Adult longhair cat with chronic abdominal wet FIP. The cat was in acceptable health except for mild weight loss, lethargy, poor coat quality, and occasional low-grade fever. Abdominal distension was not noted for some time, and the abdominal fluid contained relatively low protein and white blood cell counts.
Figure 9. A young cat who presented with rapid onset of high fever, loss of appetite, abdominal distension and abdominal fluid with a high protein and white blood cell content.
Most cats with dry FIP present with disease symptoms limited to the abdomen and/or chest. The most common clinical signs of dry FIP are palpable or ultrasound-identifiable masses in the kidney (Fig. 4), cecum, colon, liver, and associated lymph nodes (Fig. 5). Lesions of dry FIP usually spare the thoracic cavity and rarely occur in the skin, nasal passages, pericardium, and testes as part of a wider systemic disease.
Neurological and ocular disease are the sole or secondary features of 10 % of all FIP cases and are 10 times more often associated with dry than wet FIP (Pedersen 2009). The neurological and ocular forms of FIP have been classified as forms of dry FIP, but it may be more appropriate to classify them as distinct forms of FIP resulting from the modifying effects of the blood-ocular and blood-brain barriers behind which they occur. These barriers have a strong impact on the nature of eye and central nervous system (CNS) disease and response to antiviral therapy.
Clinical signs of neurologic FIP involve both the brain and spinal cord and include posterior weakness and ataxia, generalized incoordination, seizures, mental dullness, anisocoria, and varying degrees of fecal and/or urinary incontinence (Foley et al., 1998; Dickinson et al., 2020) ( Fig. 10). Extreme intracranial pressure can lead to sudden herniation of the cerebellum and brainstem into the spinal canal and spinal shock syndrome. Prodromal symptoms include compulsive wall or floor licking, litter eating, involuntary muscle twitching, and reluctance or inability to jump to high places. Eye involvement may precede or accompany neurological disease. Neurological FIP is a common phenomenon with antiviral therapy, either occurring during treatment of non-CNS forms of FIP or as a manifestation of disease relapse after treatment cessation (Pedersen et al., 2018, 2019; Dickinson et al., 2020).
Figure 10. A young cat with dry FIP and neurological impairment. The cat is lethargic, emaciated and with poor fur. The fur in the perineal area is wet and stained from urinary incontinence.
Figure 11. This cat's right iris staining was the first sign of FIP-associated uveitis. There is a slight haze in the anterior chamber, and there are fibrin deposits rich in red blood cells on the inside of the cornea. The pupils are also unequal (anisocoria).
Figure 12. A young cat with ocular FIP presenting as anterior uveitis in the right eye with secondary glaucoma causing globe enlargement. The iris has changed color due to inflammation, the vessels at the base of the iris are congested, and there is turbidity of aqueous humor and inflammatory products on the back of the cornea. Intraocular pressure is usually low in uncomplicated uveitis but elevated in cats with glaucoma.
Figure 13. This young cat had anterior uveitis, but her FIP therapy with GS-441524 was delayed, allowing glaucoma to develop in both eyes. Treatment cleared the underlying uveitis and greatly improved external health, but secondary glaucoma and blindness persisted.
Eye involvement is usually obvious and is confirmed by ophthalmoscopic examination of the anterior and posterior chambers. Ocular FIP affects the iris, ciliary bodies, retina, and optic disc to varying degrees (Peiffer and Wilcock, 1991; Ziółkowska et al., 2017; Andrew, 2000). The earliest symptom is often a unilateral change in the color of the iris (Fig. 11). The anterior chamber may appear cloudy and may show high protein levels and water turbidity on refraction. Inflammatory products in the form of activated macrophages, red blood cells, fibrin markers and small blood clots are washed into the anterior chamber. This material often adheres to the back of the cornea as keratic precipitates (Fig. 12). The disease can also affect the retina in tapetal and non-tapetal areas and lead to retinal detachment. Intraocular pressure is usually low, except in cases complicated by involvement of the ciliary body and glaucoma (Fig. 12, 13).
FIP Diagnosis
Signaling, environmental history, clinical signs, and physical examination findings often point to FIP (Tasker, 2018). A thorough physical examination should include body weight and temperature, coat and body condition, manual palpation of the abdomen and abdominal organs, gross assessment of cardiac and pulmonary function, and a cursory examination of the eyes and neurological system. Strong suspicion of an effusion in the abdominal or thoracic cavity may warrant confirmatory aspiration and even in-house fluid analysis as part of the initial examination.
Abnormalities in the complete blood count (CBC) and basic serum biochemical panel are important factors in the diagnosis of FIP (Tasker, 2018; Felten and Hartmann, 2019) and monitoring of antiviral therapy (Pedersen et al., 2018, 2019; Jones et al., 2021). ; Krentz et al., 2021) (Fig. 14). Total leukocyte counts are most likely high in cats with wet FIP, but low counts can occur with severe inflammation. A high leukocyte count is often associated with neutrophilia, lymphopenia, and eosinopenia. Mild to moderate non-regenerative anemia is also frequently seen in both wet and dry FIP. Total protein is usually elevated due to elevated globulin levels, while albumin values tend to be low (Fig. 14). This results in an A:G ratio that is often lower than 0.5-0.6 and is considered one of the most consistent indicators of FIP. However, a low A:G ratio can occur in situations where both albumin and globulin are within the reference range or in other diseases. Therefore, the A:G ratio should not be the only FIP indicator and should always be evaluated in the context of other FIP indicators (Tasker, 2018; Felten and Hartmann, 2019). Serum protein values obtained from most serum chemistry panels are usually adequate. Serum protein electrophoresis can provide additional information, especially if protein values from serum chemistry are questionable (Stranieri et al., 2017).
Figure 14. Complete blood count (CBC) (a) of a young cat with acute wet abdominal FIP. Although the leukocyte count was not elevated, relative but not absolute neutrophilia, relative and absolute lymphopenia, relative and absolute eosinopenia, and unresponsive anemia were noted, indicated by low red blood cells, hematocrit, and hemoglobin with a normal reticulocyte count.
Figure 14. Serum biochemical examination (b) of a young cat with acute wet abdominal FIP. Relevant values in the serum chemistry panel were elevated total protein, low albumin, high globulin, low albumin/globulin (A:G) ratio, and elevated total and direct bilirubin. Liver enzymes were normal except for mildly elevated AST and BUN and creatinine were normal, indicating the absence of significant liver or kidney disease. Globulin values are not always given, but a reasonable estimate can be calculated by subtracting the albumin level from the total protein.
Overreliance on CBC and serum biochemistry abnormalities can lead to diagnostic uncertainty when absent, despite the fact that no test value is consistently abnormal in all cases of FIP (Tasker, 2018)1. The biggest differences are between the clinical form of the disease, with leukocytosis and lymphopenia being more common in cats with wet than with dry FIP (Riemer et al., 2016). Hyperbilirubinemia is common in cats with FIP, but especially in cats with wet FIP (Tasker, 2018). The author also found that many cats with primary neurological FIP show minor or no blood abnormalities. Blood test values for FIP also vary from study to study (Tasker, 2018).
A complete analysis of the effusion is important to diagnose wet FIP and to rule out other potential causes of fluid accumulation (Dempsey and Ewing, 2011). It includes color (clear or yellow), viscosity (thin or viscous), presence of precipitates, ability to form a partial clot on standing, protein content, leukocyte count, and differential. The nature of the fluid may vary depending on the duration of the disease and its severity. Effusions in cats with more severe disease usually have protein values close to serum values, are more viscous, contain more leukocytes, are more yellow in color, and have a greater ability to form partial clots on standing. Chronic effusions tend to be less inflammatory in nature, with lower protein and leukocyte counts, less viscous and clearer. These values can be determined on the spot in most clinics. The clotting factor is determined by comparing the fluid collected in the serum and in the anticoagulant tubes after standing. Color and viscosity can be approximated and protein levels can be estimated using a handheld refractometer to determine total solids. Cells are pelleted from the fluid and analyzed on a fast-stained slide using light microscopy, and the leukocyte count and differential are estimated. Cells include nonseptic neutrophils, small and medium-sized mononuclear cells, and large vacuolated macrophages (Fig. 15). It is important to note that effusions can occur in a variety of conditions, such as heart failure, cancer, hypoproteinemia, and bacterial infections. Effusions in these other diseases usually have different identifying features.
Figure 15. Stained smear of peritoneal cells centrifuged from the abdominal fluid of a cat with wet FIP and examined on a fast-stained slide by light microscopy. The predominant cells are large strongly vacuolated macrophages, smaller differentiated activated monocytes and neutrophils. The greatest concentration of viral particles is in the intracytoplasmic vacuoles of macrophages (arrows).
Figure 16. Positive result of the Rivalt test. A small sample of abdominal or thoracic fluid is carefully dropped into a small beaker filled with diluted acetic acid (8 ml of distilled water and 1 drop of concentrated acetic acid). Inflammatory proteins almost immediately precipitate and sink to the bottom (positive). Less inflammatory fluids will form diffuse precipitates (questionable) or diffuse freely in solution (negative).
A positive Rivalt test on abdominal or chest fluid is often used to diagnose FIP as a cause of effusion, and a negative test tends to rule it out (Fischer et al., 2010) (Fig. 16). However, the test may be positive in inflammatory effusions of another cause and negative in some cats with FIP. Therefore, Rivalt's test is most helpful in combination with other clinical findings of FIP and should not replace a thorough fluid analysis (Felten and Hartmann, 2019).
Serum total and direct bilirubin levels are often elevated, especially in cats with wet FIP (Fig. 14), and may be associated with jaundice and bilirubinuria. Hyperbilirubinemia in FIP is not caused by liver disease (Tasker, 2018), but rather by vasculitis, microhemorrhage, hemolysis, and destruction of damaged red blood cells by macrophages locally and in the liver. The released hemoglobin is finally metabolized to bilirubin, which is then conjugated in the hepatocytes and excreted in the urine. Glucuronidation is essential for bilirubin excretion, and genetic disorders affecting glucuronidation in humans prevent its excretion (Kalakonda et al., 2021). Cats as a species are deficient in the enzymes required for glucuronidation, making it difficult to excrete substances such as bilirubin (Court and Greenblatt 2000).
Although FIP can affect the kidneys and liver, it is not severe enough to cause significant loss of kidney or liver function. However, serum tests for blood urea nitrogen (BUN) and creatinine as indicators of kidney disease and alanine aminotransferase (ALT), alkaline phosphatase (ALP), and gamma glutamyltransferase (GGT) as indicators of liver disease are often mildly elevated in cats with FIP, especially with a more acute and serious disease (Fig. 14). Therefore, slightly abnormal test values should not be interpreted excessively if other clinical signs of liver or kidney disease are not present, while their significant increase should point to the possibility of concurrent and possibly predisposing diseases of these organs.
Serum can also be tested for other markers of systemic inflammation, such as increased levels of alpha-1-acid glycoprotein (AGP) (Paltrinieri et al., 2007) and feline serum amyloid A (fSAA) (Yuki et al., 2020). They may also prove useful in monitoring response to antiviral therapy (Krentz et al., 2021).
Radiography can be helpful in identifying chest and abdominal effusions. Abdominal ultrasound can reveal a smaller amount of effusion, identify enlarged mesenteric and ileo-cecal-colic lymph nodes, thickening of the colonic wall and lesions in organs such as the kidneys, liver and spleen (Lewis and O'Brien 2010). It may also be useful in examining the chest for lesions and assisting with needle aspiration or biopsy.
Antibody titers against FCoV have decreased since the first report nearly 50 years ago (Pedersen 1976b). The reference antibody test uses indirect fluorescent antibody staining (IFA) IFA titers ≥ 1:3200 in FIP cats are higher than most FECV-exposed cats (1:25–1:400). Newer tests often use ELISA procedures for rapid in-house or laboratory testing, but are qualitative rather than quantitative. IFA antibody titers decrease during successful antiviral treatment in many cats, but remain high in others (Dickinson et al., 2020; Krentz et al., 2021). Sequential titers can show a gradual increase in titers during the development of FIP (Pedersen et al., 1977), but previous serum samples are rarely available for comparison. Like most tests, FCoV antibody levels should not be used as the sole criterion to diagnose or rule out FIP (Felten and Hartmann, 2019) or to assess treatment success (Krentz et al., 2021).
Reverse transcriptase polymerase chain reaction (RT-PCR) is the primary means of identifying FCoV RNA in inflammatory effusions, fluids, or affected tissues (Felten and Hartmann, 2019). Accessory gene 7b RNA is present at the highest levels in tissues, fluids or exudates infected with FECV or FIPV, making it the most sensitive target for detecting low levels of virus (Gut et al., 1999). RT-PCR for FIPV S gene mutations is often used in samples that are positive for 7b RNA to be specific for FIPV (Felten et al., 2017). Other studies suggest that RT-PCR assays for FIPV-specific S gene mutations have similar specificity for FIP, but at the cost of a significant loss of sensitivity (Barker et al., 2017). A decrease in sensitivity is associated with an increase in the number of false negative results. False-negative RT-PCR tests also occur in samples that do not contain sufficient numbers of infected macrophages or in cats with very low levels of virus. False-negative results are especially common when testing whole blood.
Immunohistochemistry (IHC) detects feline coronavirus nucleocapsid protein in formalin-fixed tissues with high sensitivity and specificity, but is not as popular as RT-PCR (Litster et al., 2013; Ziółkowska et al., 2019). Specimens for IHC must contain intact infected macrophages (Fig. 17), which requires careful separation of cells from effusions and mounting them on slides, or formalin-fixed, paraffin-embedded diseased tissues that show lesions compatible with FIP. The coronavirus antigen in macrophages within a typical FIP lesion or fluid is seen only in FIP, giving IHC a high level of specificity.
Figure 17. Histological section from the thickened colon of a cat with the intestinal form of FIP. The thickened wall contained foci of macrophages (square area), which stained positive (brown-red) for FIPV nucleocapsid protein by immunoperoxidase.
A thorough ophthalmological examination is necessary to diagnose the characteristic changes of FIP (Pfeiffer and Wilcock 1991; Andrew, 2000). A sample of aqueous humor from the anterior chamber of an inflamed eye may also be useful for cytology, PCR and IHC.
Neurological FIP is often diagnosed using contrast-enhanced magnetic resonance imaging (MRI) and is often associated with cerebrospinal fluid (CSF) analysis (Crawford et al., 2017; Tasker, 2018; Dickinson et al., 2020). However, these are expensive procedures that are not always available and carry a certain risk for the cat. MRI lesions include obstructive hydrocephalus, syringomyelia, and herniation of the foramen magnum with contrast enhancement of the meninges of the brain and spinal cord and ependyma of the third ventricle, mesencephalic aqueduct, and brainstem. CSF shows an increased number of proteins and cells (neutrophils, lymphocytes, monocytes/macrophages) and, if present, can be reliable material for PCR or IHC examination.
Neurologic and/or ocular forms of FIP are often confused with systemic feline toxoplasmosis, and many cats with FIP are empirically treated for toxoplasmosis before a diagnosis of FIP is made. Fortunately, the availability of effective treatment for FIP has curtailed this practice. Systemic toxoplasmosis is much less prevalent than FIP, and fewer than 1 % cats with FIP were serologically positive in one field study.1 Therefore, testing or treatment for toxoplasmosis should only be considered once FIP has been adequately diagnosed.
Antiviral treatment as a diagnostic tool
Figure 18. A cat with FIP at the start of treatment with GS-441524 (a) and after 1 week (b). The answer is quick, the fever will disappear within 24-48 hours and the general state of health will improve significantly within 1-2 weeks. This type of response is often used to confirm a diagnosis of FIP.
Situations commonly occur where clinical findings point to FIP but doubts remain. Then there is a choice of performing several diagnostic tests, which may not lead to a more definitive diagnosis. An alternative diagnostic approach is treatment with a suitable antiviral for 1-2 weeks in the correct dose for the suspected form of FIP.2 Treatment often produces clinical improvement in as little as 24-48 hours and this rapidly progresses over the next 2 weeks and the total duration of treatment (Fig. 18). No response to test treatment and/or deterioration in health would indicate the need for further investigation of the cause(s) of ill health.
FIP Treatment
Before 2017, there was no cure for FIP, and treatment was mainly aimed at alleviating the symptoms of the disease (Izes et al., 2020). Such supportive treatment was aimed at maintaining good nutrition, controlling inflammation (corticosteroids), changing immune responses (interferons, cyclophosphamide, chlorambucil) and inhibiting key cytokine responses (pentoxifylline and other TNF-alpha inhibitors). Nutritional supplements that were supposed to help specific organ functions were also commonly used, such as one (Polyprenyl Immunostimulant) that was supposed to improve immunity and prolong survival in cats with dry but not wet FIP (Legendre et al., 2017). The effect of good supportive care on survival could not be determined because most cats were euthanized after diagnosis or within days or weeks. The survival rate for even the mildest forms of dry FIP and the most permanent treatment in one study was only 13 % at 200 days and 6 % at 300 days (Legendre et al., 2017).
Many commercially available drugs and compounds inhibit FIPV infection or replication in vitro, some of which are drugs known to inhibit specific HIV or hepatitis C proteins, while others work by inhibiting normal cellular processes that the virus usurps for its own life cycle (Hsieh et al., 2010; Izes et al., 2020; Delaplace et al., 2021). These various drugs and agents include cyclosporine and related immunophilins, several nucleoside and protease inhibitors, vioporin inhibitors, pyridine N-oxide derivatives, chloroquine and related compounds, ivermectin, several plant lectins, ubiquitin inhibitors, itraconazole, and several antibiotics. However, the concentrations required to inhibit viral replication in vitro often approach toxic values for cells. It has also been difficult to transfer favorable in vitro conclusions to animals, and studies in sick cats have rarely followed. Ribavarin inhibits FIPV replication in vitro, but was not effective as a treatment for experimental FIP (Weiss et al., 1993). The efficacy of chloroquine was tested in laboratory cats infected with FIPV, but clinical outcomes in treated cats were only slightly better than untreated ones and hepatotoxicity was demonstrated (Takano et al., 2013). A 3-month-old kitten with chest wet FIP treated with itraconazole and prednisolone developed neurological FIP and was euthanized after 38 days of treatment (Kameshima et al., 2020). Mefloquine also inhibited FIPV replication at low concentrations in cultured feline cells without cytotoxic effects, and preliminary pharmacokinetic studies in cats appeared favorable (Yu et al., 2020), but evidence of its safety and efficacy in clinical trials in cats with FIP has yet to be established. published.
A breakthrough in the treatment of FIP occurred in 2016-2019 when antiviral drugs were reported that target specific FIPV proteins essential for replication. The first of these drugs was GC376, a major protease inhibitor (Mpro ) FIPV (Kim et al., 2016; Pedersen et al., 2018). Protease inhibitors prevent the formation of individual viral proteins by inhibiting their cleavage from polyprotein precursors. GC376 was able to cure all experimentally infected cats and 7 of 21 cats with naturally occurring wet and dry FIP, but was less effective for cats with ocular or neurological signs (Pedersen et al., 2018). The second of these drugs was GS-441514, the active part of the prodrug remdesivir (Gilead Sciences; Murphy et al., 2018; Pedersen et al., 2019). GS-441524 is an adenosine nucleoside analog that blocks FIPV replication by inserting a nonsense adenosine into the developing viral RNA. GS-441524 was also able to cure all experimentally infected cats (Murphy et al., 2018) and 25/31 cats with naturally occurring wet and dry FIP (Pedersen et al., 2019). It has also been shown to be effective at higher doses in several cats with ocular and neurological FIP (Pedersen et al., 2019) and is now the drug of first choice for cats with neurological FIP (Dickinson et al., 2020). GS-441524 has cured thousands of FIP cats from around the world over the past three years, with an overall cure rate of just over 90 % (Jones et al., 2021).1
Although the ability of GC376 and GS-441524 to treat cats has been known for several years, neither is currently legally available in most countries. The rights to GC376 have been purchased by Anivive, but it has not yet been launched.3 Potential conflicts with the development of remdesivir for the treatment of COVID-19 in humans led Gilead Sciences to withhold rights to GS-441524 for animal use, prompting the creation of an unapproved source for GS-441524 from China (Jones et al, 2021).1,2,4 Remdesivir is rapidly metabolized in the body to GS-441524 and has been approved for the treatment of FIP in some countries.2 GS-441524 can also be administered orally in higher doses and is currently commonly used in practice (Krentz et al., 2021).1
The efficacy of drugs such as GC376 and GS-441524 on FIP cats, the use of which preceded the COVID-19 pandemic, has been recognized by researchers investigating related SARS-CoV 2 inhibitors (Yan et al., 2020; Vuong et al., 2021). Remdesivir, an injectable drug called glaucoma (Gilead), has been used worldwide to reduce mortality from COVID-19 (Beigel et al., 2020). GC373, the active form of the prodrug GC376, has undergone simple modifications to increase efficacy and oral bioavailability (Vuong et al., 2021). The GC373-related drug, nirmatrelvir, has been successfully tested against early COVID-19 infections and has been approved for the treatment of early COVID-19 and marketed as paxlovid (Pfizer). Paxlovid consists of two medicines, nirmatrevir and the HIV protease inhibitor ritonavir. Ritonavir is not a significant inhibitor of SARS-CoV 2, but is reported to prolong the half-life of Mprowhen used in combination (Vuong et al., 2020). Nirmatrelvir and paxlovid have not been tested in cats with FIP at present, but based on experience with the closely related drug GC376, oral treatment of some forms of FIP may be important in the future.
Two other nucleoside analogs, EIDD-1931 and EIDD-2801 (Painter et al., 2021), have been investigated for the treatment of multiple RNA virus infections in humans and animals. EIDD-1931 is the experimental designation for beta-D-N4-hydroxycytidine, a compound widely studied since the 1970's. Beta-D-N4-hydroxycytidine is metabolized to a ribonucleoside analog, which is incorporated into RNA instead of cytidine and leads to fatal mutations in the viral RNA strand. The compound is an inhibitor of a wide variety of human and animal RNA viruses, including all known coronaviruses. EIDD-1931 was modified to increase oral absorption and was termed EIDD-2801 (molnupiravir) (Painter et al., 2021). Molnupiravir is deesterified in the body to its active ingredient, beta-D-N4-hydroxycytidine. Therefore, EIDD-1931 and molnupiravir are analogous to GS-441524 and remdesivir. Molnupiravir is marketed for the home treatment of primary COVID-19 under the names Lagevrio (Merck, USA) or Molnulup (Lupine, India).
Both EIDD-1931 and EIDD-2801 have been shown to be effective in inhibiting FIPV in tissue culture (Cook et al., 2021), and EIDD-2801 is currently used to treat some cases of FIP in the field.5,7 The effective concentration of 50 % (EC50) for EIDD-1931 against FIPV is 0.09 µM, EIDD-2801 0.4 µM and GS-441524 0.66 µM (Cook et al., 2021). The percentage cytotoxicity at 100 μM for these compounds is 2.8, 3.8 and 0.0. Thus, EIDD-1931 and -2801 are slightly more inhibitory to viruses, but more cytotoxic than GS-441524. Resistance to GS-441524 has been reported in some cases of FIP (Pedersen et al., 2019) and to remdesivir in patients with COVID-19 (Painter et al., 2021), but these isolates remain sensitive to molnupiravir (Sheahan et al., 2020). This may prove useful in combating resistance to GS-441524 in cats and humans and in developing multidrug therapy to prevent the development of resistance.
What will full approval of medicines like molnupiravir and paxlovid mean for cats? Full human approval should allow veterinarians in most countries to legally procure medicinal products authorized for human consumption for direct use in animals, provided that the guidelines for use in non-food producing animals are followed.6 This requires a reformulation of a medicine made for humans and purchased at a price for humans. Hopefully, antivirals similar or identical to those approved for humans will be licensed exclusively for animals and sold at a much lower price, but this is likely to take years.
Commercial and policy issues that limit the current use of antivirals such as GS-441524 in animal diseases such as FIP are for current cat owners and feline support groups who have already bypassed the current drug approval system and its emphasis on overriding human needs, irrelevant (Jones et al., 2021; Krentz et al., 2021). Advocates of FIP treatment are currently found around the world and often associate under the expanded FIP Warrior brand. Members of these groups often act as intermediaries between owners, veterinarians and antiviral suppliers and often provide advice to those who are unable to obtain veterinary treatment assistance. Some of these groups, such as FIP Warriors Czech Republic / Slovakia7, have placed their experience with FIP treatment on the Internet, where they provide much-needed information about current antiviral treatment.
Current situation of FIP treatment
The current drug of choice for the treatment of FIP is the adenosine nucleoside analog GS-441524, which was first published in the scientific literature under experimental conditions (Murphy et al., 2018) and later against naturally occurring disease (Pedersen et al., 2019). Although initial experimental and field studies of GS-441524 were conducted in collaboration between researchers at Gilead Sciences and the University of California, Davis, the relationship between Remdesivir and GS-441524 and the onset of the COVID-19 pandemic in 2019 led Gilead Sciences to eventually did not grant rights to use GS-441524 to animals on the grounds that it could interfere with the development of Remdesivir for human use.4 Objections to this decision have been raised directly by the company and in several internet forums.4 Subsequent pressure from cat owners, cat rescue groups and cat lovers, along with opportunistic Chinese drug manufacturers, quickly created an alternative unapproved source of GS-441524, its market and treatment network.4 This network has largely bypassed veterinarians, most of whom have decided to wait for the drug to be legalized (Jones et al., 2021). The result of this relationship was an almost seamless transition of FIP treatment with GS-441524 from the laboratory to a rapidly expanding worldwide network of groups, under the umbrella of FIP Warriors (Jones et al., 2021).4,7
The sale and use of GS-441524 in practice for the treatment of FIP began almost immediately with the first publication of the results of field trials (Pedersen et al., 2019) (Fig. 19).
Figure 19. Graph of the monthly development of treatment of cats from the Czech Republic and Slovakia since August 2019. This graph comes from the FIP Warrior CZ / SK website.1 These figures reflect the experiences of other FIP Warrior groups around the world. Since 2019, when the first field study GS-441524 was published (Pedersen et al. 2019), thousands of cats have been successfully treated for FIP worldwide. The winter peaks of the disease reflect a late spring and summer increase in the number of kittens born and a high incidence of FIP, which usually begins at 3 to 6 months of age (Fig. 6). This chart is from the FIP Warrior CZ / SK website.1
Figure 20. The main participants in the GS-441524 treatment. This chart is from the FIP Warriors CZ / SK website.1
The fact that GS-441524 is not legally approved for use in animals has prevented many veterinarians from recognizing or participating in this treatment. Only 25 % cats in the CZ / SK treated group received veterinary support during treatment (Fig. 20), although more veterinarians may have been involved in the diagnosis of the disease. Interestingly, this number was higher than the 8.7 % treated cats in the United States that received veterinary care (Jones et al., 2021). However, participants in CZ / SK studies and similar groups around the world are not without medical experience, as many of them are engaged in temporary care / rescue and have had considerable direct and indirect veterinary experience with cat diseases and their treatment and castration programs.
From the first laboratory studies and research of Chinese manufacturers, it was known that GS-441524 can be absorbed orally, although with less efficiency (Kim et al. 2016).9 The first sellers of GS-441524 further investigated this fact and found that effective blood levels could be achieved by increasing the amount administered orally compared to injection.8 Supplements have often been added to GS-441524 oral capsules or tablets, claiming that they increase absorption or have additive therapeutic benefits (Krentz et al., 2011). Most major retailers of GS-441524 now offer oral versions, and oral therapy is becoming increasingly popular either as a single treatment or in combination with GS-441524 (Figure 21). The success of GS-441524 oral therapy did not differ significantly from GS-441524 injection therapy (Figure 22).
Figure 21. Comparison of the use of oral (tablets or capsules) and injectable (subcutaneous) forms of GS-441524 for the treatment of FIP in cats from the Czech Republic and Slovakia. This chart is from the FIP Warriors CZ / SK website.1
Figure 22. There is no significant difference in treatment success with oral administration of GS-441524 compared to subcutaneously administered GS, but the actual amount (mg) of drug administered orally in each dose is up to twice the amount contained in the same dose of GS injection. This chart is from the FIP Warriors CZ / SK.1 website
The recommended dosing schedule for GS-441524 based on published data from field studies (Pedersen et al., 2019) was 4 mg / kg, subcutaneous (SC), daily (q24h), ie 4 mg / kg, SC, q24h. This recommended starting dose for cats with wet or dry FIP without ocular or neurological symptoms tended to increase to 6 mg / kg SC q24h over time (Fig. 23). 8 mg / kg SC q24h is the current recommended dose for cats with ocular symptoms and 10 or 12 mg / kg SC q24h for cats with neurological symptoms.
Figure 23. Daily dose of GS-441524, which was used to treat FIP in cats from the Czech Republic and Slovakia. The usual starting dose was 6 mg / day, with some cats requiring higher doses based on response to treatment, form of the disease and recurrence after treatment appeared to be successful. GS-441524 oral formulations are usually labeled to match the dosage used for the injectable drug, but contain up to twice the labeled amount. This chart is from the FIP Warrior CZ / SK website.1
The optimal duration of treatment, as determined in the initial clinical study, is 84 days (Pedersen et al., 2019). In some cases of acute wet FIP in younger cats, healing has been achieved in 6-8 weeks, but some cats need more than 84 days. As shown in Figure 24.72 % cats were treated for 81-90 days, 19 % longer and only 9 % were treated shorter. Unfortunately, there is no simple and accurate test to determine the moment of cure, and the decision to stop treatment is based on a complete return to health and normal blood test values. Cats treated for much longer than 100 days were usually those requiring a GS dose higher than 12 mg / kg per day by injection or equivalent oral dose, cats that relapsed during the 12-week post-treatment observation period, cats with neurological disease or cats that have become resistant to GS-441524.
Figure 24. Duration of treatment with GS-141524 in 352 cats successfully treated for all forms of FIP. This chart is from the FIP Warriors CZ / SK website.1
Figure 25. Initial treatment was successful in 88.1 % cats and 6.2 % cats died or were sacrificed either due to insufficient response to treatment, financial reasons or treatment side effects. Another 5.7 % cats relapsed after initial treatment and approximately the same number of cats either recovered or died after further treatment. This chart is from the FIP Warriors CZ / SK.1 website
The treatment success rate for all forms of FIP in cats from the Czech Republic and Slovakia is 88.1 % in the first treatment, but when cats that relapsed after the first treatment and recovered after the second treatment (3.1 %) were included, the overall success rate was more as 91 % (Fig. 25). This cure rate is identical to the cure rate of other groups of FIP fighters (Jones et al., 2021). Treatment success did not differ between cats with wet or dry FIP and without ocular or neurological impairment (Fig. 26). However, the cure rate in cats with ocular and neurological impairments was lower, at 80 % compared to 92 % in all other forms of FIP (Fig. 26).
Figure 26. Cure rate of cats with wet or dry FIP without ocular or neurological symptoms and cats with ocular or neurological disease as the main feature of their disease. This chart is from the FIP Warriors CZ / SK website.1
Figure 27. The condition of the cats one year after the successful completion of treatment with GS-441524. This chart is from the FIP Warriors CZ / SK website.1
Cats that have been successfully treated for FIP have been followed for 4 to 5 years, including cases reported in the first field studies. There have been no recurrences or recurrent cases of FIP in this group of first field trials. Data on annual survival are available from a much larger population of the CZ / SK study, which shows that 90.5 % cats are still healthy one year after the end of treatment (Fig. 27). Only 1.3 % of these cats died from causes other than FIP and 8.2 % cohort is currently in an unknown medical condition. The low proportion of cats that died of unknown causes within a year of treatment and their positive response to treatment suggest that FIP has been diagnosed correctly.
EIDD-2801 (molnupiravir) is currently being used in the field for the main treatment and for the treatment of GS-441524-resistant cats.5,7,9 EIDD-1931, the active form of EIDD-2081, needs to be further researched because it is no longer covered by patent protection and is thus easily approved for use in animals if it is found to be truly safe and effective.5 Nirmatrelvir, an oral form of GC373 and a closely related GC376, still needs to be studied for the treatment of FIP.
Acknowledgement
I am indebted to Ladislav Mihok and his collaborators at “FIP Warriors Czech Republic/Slovakia” for allowing me to share data from their website. This website contains the most significant, thorough and organized collection of data on the treatment of FIP with antivirals to date. The website also contains useful information and advice on initiating, managing and monitoring current treatment. The collection of cats and their data is continuously and regularly updated and at the time of writing included over 600 cats with FIP.
References
Addie DD, Toth S, Murray GD, Jarrett O, 1995. Risk of feline infectious peritonitis in cats naturally infected with feline coronavirus. American Journal of Veterinary Research, 56, 429-34.
Addie DD, Schaap IA, Nicolson L, Jarrett O, 2003. Persistence and transmission of natural type I feline coronavirus infection. Journal of General Virology 84, 2735–2744.
Andrew SE, 2000. Feline infectious peritonitis. Veterinary Clinics of North America and Small Animal Practice 30, 987-1000.
Barker EN, Stranieri A, Helps CR, Porter EL, Davison AD, Day MJ, Knowles T, Kipar A, Tasker S, 2017. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Veterinary Research 48, 60.
Beigel JH, Tomashek KM, Dodd LE, Mehta EK, Zingman BS, et al., 2020. Remdesivir for the Treatment of Covid-19 - Final Report. New England Journal of Medicine, 383, 1813-1826,
Bubenikova J, Vrabelova J, Stejskalova K, Futas J, Plasil M, Cerna P, Oppelt J, Lobova D, Molinkova D, Horin P, 2020. Candidate gene markers associated with fecal shedding of the feline enteric coronavirus (FECV). Pathogens 9, 958.
Cassado Ados A, D'Império Lima, Bortoluci KR., 2015. Revisiting mouse peritoneal macrophages: heterogeneity, development, and function. Frontiers in Immunology 6, 225.
Cave TA, Thompson H, Reid SW, Hodgson DR, Addie DD, 2002. Kitten mortality in the United Kingdom: a retrospective analysis of 274 histopathological examinations (1986 to 2000). Veterinary Record 151, 497–501.
Cook SE, Vogel H, Castillo D, Olsen M, Pedersen N, Murphy BG, 2021. Investigation of monotherapy and combined anticoronaviral therapies against feline coronavirus serotype II in vitro. Journal of Feline Medicine and Surgery. doi: 10.1177 / 1098612X211048647. Epub ahead of print. PMID: 34676775.
Cornelissen E, Dewerchin HL, Van Hamme E, Nauwynck HJ, 2007. Absence of surface expression of feline infectious peritonitis virus (FIPV) antigens on infected cells isolated from cats with FIP. Veterinary Microbiology. 121, 131-137,
Cotter SM, Gilmore CE, Rollins C. 1973, Multiple cases of feline leukemia and feline infectious peritonitis in a household. Journal of the American Veterinary Medical Association 162, 1054–1058.
Court MH., Greenblatt DJ. 2000, Molecular genetic basis for deficient acetaminophen glucuronidation by cats: UGT1A6 is a pseudogene, and evidence for reduced diversity of expressed hepatic UGT1A isoforms Pharmacogenetics, 10, 355-369
Crawford AH, Stoll AL, Sanchez-Masian D, Shea A, Michaels J, Fraser AR, Beltran E, 2017. clinicopathologic features and magnetic resonance imaging findings in 24 cats with histopathologically confirmed neurologic feline infectious peritonitis. Journal of Veterinary Internal Medicine 31, 1477–1486.
Day MJ, 2010. Aging, immunosenescence and inflammageing in the dog and cat. Journal of Comparative Pathology 142 Suppl 1, S60-69.
Delaplace M, Huet H, Gambino A, Le Poder S, 2021. Feline coronavirus antivirals: A review. Pathogens 10, 1150. doi: 10.3390 / pathogens10091150.
Dempsey SM, Ewing PJ, 2011. A Review of the Pathophysiology, Classification, and Analysis of Canine and Feline Cavitary Effusions. Journal of the American Animal Hospital Association 47, 1–11.
de Sousa JR, Sotto MN, Simões Quaresma JA, 2017. Leprosy as a complex infection: Breakdown of the Th1 and Th2 immune paradigm in the immunopathogenesis of the disease. Frontiers in Immunology 8,1635.
Dewerchin HL, Cornelissen E, Van Hamme E, Smits K, Verhasselt B, Nauwynck HJ, 2008. Surface-expressed viral proteins in feline infectious peritonitis virus-infected monocytes are internalized through a clathrin- and caveolae-independent pathway. Journal of General Virology 89, 2731–2740
Dewerchin HL, Desmarets LM, Noppe Y, Nauwynck HJ, 2014. Myosins 1 and 6, myosin light chain kinase, actin and microtubules cooperate during antibody-mediated internalization and trafficking of membrane-expressed viral antigens in feline infectious peritonitis virus infected monocytes. Veterinary Research 45, 17.
Dickinson PJ, Bannasch M, Thomasy SM, Murthy VD, Vernau KM, Liepnieks M, Montgomery E, Knickelbein KE, Murphy B, Pedersen NC, 2020. Antiviral treatment using the adenosine nucleoside analogue GS ‐ 441524 in cats with clinically diagnosed neurological feline infectious peritonitis. Journal of Veterinary Internal Medicine 34, 1587–1593.
Drechsler Y, Alcaraz A, Bossong FJ, Collisson EW, Diniz PP, 2011. Feline coronavirus in multicat environments. Veterinary Clinics North America and Small Animal Practice41, 1133-1169.
Fankauser R, Fatzer R, 1997. Meningitis and chorioependymitis granulomatosa der Katze. Possible conditions for infectious peritonitis (FIP). Client Practice 22, 19–22.
Felten S, Leutenegger CM, Balzer HJ, Pantchev N, Matiasek K, Wess G, Egberink H, Hartmann K, 2017. Sensitivity and specificity of a real-time reverse transcriptase polymerase chain reaction detecting feline coronavirus mutations in effusion and serum / plasma of cats to diagnose feline infectious peritonitis. BMC Veterinary Research 13, 228.
Felten S, Hartmann K, 2019. Diagnosis of Feline Infectious Peritonitis: A Review of the Current Literature. Viruses 11, 1068.
Fischer Y, Sauter-Louis C, Hartmann K, 2012. Diagnostic accuracy of the Rivalta test for feline infectious peritonitis. Veterinary Clinical Pathology 41, 558–67.
Foley JE, Poland A, Carlson J, Pedersen NC, 1997. Risk factors for feline infectious peritonitis among cats in multiple-cat environments with endemic feline enteric coronavirus. Journal of the American Veterinary Medicine Association 210, 1313-1318.
Foley JE, Lapointe JM, Koblik P, Poland A, Pedersen NC, 1998. Diagnostic features of clinical neurologic feline infectious peritonitis. Journal of Veterinary Internal 12, 415–423.
Gaskell RM, Povey RC, 1977. Experimental induction of feline viral rhinotracheitis virus re-excretion in FVR-recovered cats. Veterinary Record 100, 128–133.
Golovko L, Lyons LA, Liu H, Sørensen A, Wehnert S, Pedersen NC, 2013. Genetic susceptibility to feline infectious peritonitis in Birman cats. Virus Research 175, 58–63.
Gunn-Moore DA, Gaunt C, Shaw DJ, 2012. Incidence of mycobacterial infections in cats in great britain: estimate from feline tissue samples submitted to diagnostic laboratories. Transboundary and Emerging Diseases. 60, 338-344.
Gut, M, Leutenegger, CM, Huder, JB, Pedersen NC, H, 1999. One-tube fluorogenic reverse transcription-polymerase chain reaction for the quantitation of feline coronaviruses. Journal of Virological Methods 77, 37–46.
Hardy WD Jr., 1981. Feline leukemia virus non-neoplastic diseases. Journal of the American Animal Hospital Association 17, 941-949.
Healey EA, Andre NM, Miller AD, Whitaker GR, Berliner EA, 2022. Outbreak of feline infectious peritonitis (FIP) in shelter-housed cats: Molecular analysis of the feline coronavirus S1/S2 cleavage site consistent with a 'circulating virulent-avirulent theory' of FIP pathogenesis. Journal of Feline Medicine and Surgery Open Reports 8, 20551169221074226.
Herrewegh AAPM, Mähler M, Hedrich HJ, Haagmans BL, Egberink HF, Horzinek MC, Rottier PJM, de Groot RJ, 1997. Persistence and evolution of feline coronavirus in a closed cat-breeding colony. Virology 234, 349–363.
Herrewegh AA, Smeenk I, Horzinek MC, Rottier PJ, de Groot RJ, 1998. Feline coronavirus type II strains 79-1683 and 79-1146 originate from a double recombination between feline coronavirus type I and canine coronavirus. Journal of Virology 72, 4508–4514.
Hickman MA, Morris JG, Rogers QR, Pedersen NC, 1995. Elimination of feline coronavirus infection from a large experimental specific pathogen-free cat breeding colony by serologic testing and isolation, Feline Practice 23, 96–102.
Hsieh LE, Lin CN, Su BL, Jan TR, Chen CM, Wang CH, Lin DS, Lin CT, Chueh LL. 2010. Synergistic antiviral effect of Galanthus nivalis agglutinin and nelfinavir against feline coronavirus. Antiviral Research 88, 25–30.
Holzworth J, 1963. Some important disorders of cats. Cornell Veterinarian 53, 157–160.
Izes AM, Yu J, Norris JM, Govendir M, 2020. Current status on treatment options for feline infectious peritonitis and SARS-CoV-2 positive cats. Veterinary Quarterly 40, 322–330.
Jones S, Novicoff W, Nadeau J, Evans S, 2021. Unlicensed GS-441524-like antiviral therapy can be effective for at-home treatment of feline infectious peritonitis. Animals 11, 2257.
Kalakonda A, Jenkins BA, John S. Physiology, Bilirubin. [Updated 2021 Sep 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470290/
Mustaffa-Kamal F, Liu H, Pedersen NC, Sparger EE, 2019. Characterization of antiviral T cell responses during primary and secondary challenge of laboratory cats with feline infectious peritonitis virus (FIPV). BMC Veterinary Research 15,165.
Kameshima S, Kimura Y, Doki T, Takano T, Park CH, Itoh N, 2020. Clinical efficacy of combination therapy of itraconazole and prednisolone for treating effusive feline infectious peritonitis. Journal of Veterinary Medical Science 82, 1492–1496.
Kim Y, Liu H, Galasiti Kankanamalage AC, Weerasekara S, Hua DH, Groutas WC, Chang KO, Pedersen NC, 2016. Reversal of the progression of fatal coronavirus Infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathogens 12: e1005531.
Kipar A, May H, Menger S, Weber M, Leukert W, Reinacher M, 2005. Morphologic features, and development of granulomatous vasculitis in feline infectious peritonitis. Veterinary Pathology 42, 321–330.
Krentz D., Zenger K., Alberer M., Felten S., Bergmann M, Dorsch R., Matiasek, K., Kolberg, L., Hofmann-Lehmann, R., Meli, ML, et al., 2021. Curing cats with feline infectious peritonitis with an oral multi-component drug containing GS-441524. Viruses 13, 2228.
Legendre AM, Kuritz T, Galyon G, Baylor VM, Heidel RE, 2017. Polyprenyl immunostimulant treatment of cats with presumptive non-effusive feline infectious peritonitis in a field study. Frontiers in Veterinary Science 4, 7.
Teacher C, Lê-Bury P, Pizarro-Cerdá J, Dussurget O, 2020. Emerging Evasion Mechanisms of Macrophage Defenses by Pathogenic Bacteria. Frontiers in Cellular and Infection Microbiology, 10, 538.
Lewis KM, O'Brien RT, 2010. Abdominal ultrasonographic findings associated with feline infectious peritonitis: a retrospective review of 16 cases. Journal of the American Animal Hospital Association. 46, 152-60.
Licitra BN, Millet JK, Regan AD, Hamilton BS, Rinaldi VD, Duhamel GE, Whittaker GR, 2013. Mutation in spike protein cleavage site and pathogenesis of feline coronavirus. Emerging Infectious Diseases 19, 1066–1073.
Lin CN, Su BL, Wang CH, Hsieh MW, Chueh TJ, Chueh LL, 2009. Genetic diversity and correlation with feline infectious peritonitis of feline coronavirus type I and II: A 5-year study in Taiwan. Veterinary Microbiology 136, 233–239.
Litster AL. Pogranichniy R, Lin TL, 2013. Diagnostic utility of a direct immunofluorescence test to detect feline coronavirus antigen in macrophages in effusive feline infectious peritonitis. Veterinary Journal 198, 362–366.
Lloret A, Hartmann K, Pennisi MG, Ferrer L, Addie D, Belák S, Boucraut-Baralon C, Egberink H, Frymus T, Gruffydd-Jones T, et al., 2013. Rare systemic mycoses in cats: blastomycosis, histoplasmosis and coccidioidomycosis: ABCD guidelines on prevention and management. Journal of Feline Medicine and Surgery 15, 624–627.
Longstaff L, Porter E, Crossley VJ, Hayhow SE, Helps CR, Tasker S, 2017. Feline coronavirus quantitative reverse transcriptase polymerase chain reaction on effusion samples in cats with and without feline infectious peritonitis. Journal of Feline Medicine and Surgery 19, 240–245.
Mahase E. 2021. Covid-19: Molnupiravir reduces risk of hospital admission or death by 50% in patients at risk, MSD reports. BMJ 375, n2422.
Malbon AJ, Meli ML, Barker EN, Davidson AD, Tasker S, Kipar A, 2019. inflammatory mediators in the mesenteric lymph nodes, site of a possible intermediate phase in the immune response to feline coronavirus and the pathogenesis of feline infectious peritonitis? Journal of Comparative Pathology 166, 69–86.
Malbon AJ, Russo G, Burgener C, Barker EN, Meli ML, Tasker S, Kipar A, 2020. the effect of natural feline coronavirus infection on the host immune response: A whole-transcriptome analysis of the mesenteric lymph nodes in cats with and without feline infectious peritonitis. Pathogens 7, 524.
Mor G, Cardenas I, 2010. The immune system in pregnancy: A unique complexity. American Journal of Reproductive Immunology 63, 425–433.
Murphy BG, Perron M, Murakami E, Bauer K, Park Y, Eckstrand C, Liepnieks M, Pedersen NC, 2018. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Veterinary Microbiology 219, 226–233.
Painter WP, Holman W, Bush JA, Almazedi F, Malik H, Eraut NCJE, Morin MJ, Szewczyk LJ, Painter GR, 2021. Human safety, tolerability, and pharmacokinetics of molnupiravir, a novel broad-spectrum oral antiviral agent with activity against SARS-CoV-2. Antimicrobial Agents and Chemotherapeutics 65: e02428-20.
Paltrinieri S, Giordano A, Tranquillo V, Guazzetti S, 2007. Critical assessment of the diagnostic value of feline α1-acid glycoprotein for feline infectious peritonitis using the likelihood ratios approach. Journal of Veterinary Diagnostic Investigation. 19, 266-272.
Pearson M, LaVoy A, Evans S, Vilander A, Webb C, Graham B, Musselman E, LeCureux J, VandeWoude S, Dean GA, 2019. Mucosal Immune Response to Feline Enteric Coronavirus Infection. Viruses 11, 906.
Pedersen NC, 1976b. Serologic Studies of Naturally Occurring Feline Infectious
peritonitis. American Journal of Veterinary Research 37, 1447–1453.
Pedersen NC, 2009. A review of feline infectious peritonitis virus infection: 1963-2008. Journal of Feline Medicine and Surgery 11, 225–258.
Pedersen NC, Boyle J, 1980. Immunologic Phenomena in the Effusive Form of Feline Infectious Peritonitis. American Journal of Veterinary Research 41: 868–876.
Pedersen NC, Ward J, Mengeling WL, 1978. Antigenic relationship of the feline infectious peritonitis virus to coronaviruses of other species. Archives of Virology58, 45–53.
Pedersen NC, Allen CE, Lyons LA, 2008. Pathogenesis of feline enteric coronavirus infection. Journal of Feline Medicine and Surgery 10, 529–541.
Pedersen NC, Theilen G, Keane MA, Fairbanks L, Mason T, Orser B, Che CH, Allison C, 1977. Studies of naturally transmitted feline leukemia virus infection. American Journal of Veterinary Research 38, 1523–1531.
Pedersen NC, Boyle JF, Floyd K, Fudge A, Barker J, 1981. An enteric coronavirus infection of cats and its relationship to feline infectious peritonitis. American Journal of Veterinary Research 42, 368-377.
Pedersen NC, Meric SM, Hoe E, Johnson L. Plucker S, Theilen GH, 1982. The clinical significance of latent feline leukemia virus infection. Feline Practice 14, 32–48.
Pedersen NC, Black JW, Boyle JF, Evermann JF, McKeirnan AJ, Ott RL, 1984. Pathogenic differences between various feline coronavirus isolates. Advances in Experimental Medicine and Biology 173, 365–380.
Pedersen NC, Liu H, Dodd KA, Pesavento PA, 2009. Significance of coronavirus mutants in feces and diseased tissues of cats suffering from feline infectious peritonitis. Viruses1, 166-184.
Pedersen NC, Liu H, Durden M, Lyons LA, 2016. Natural resistance to experimental feline infectious peritonitis virus infection is decreased rather than increased by positive genetic selection. Veterinary Immunology and Immunopathology 171, 17–20.
Pedersen NC, Liu H, Scarlett J, Leutenegger CM, Golovko L, Kennedy H, Kamal FM, 2012. Feline infectious peritonitis: role of the feline coronavirus 3c gene in intestinal tropism and pathogenicity based upon isolates from resident and adopted shelter cats. Virus Research 165,17-28
Pedersen NC, Kim Y, Liu H, Galasiti Kankanamalage AC, Eckstrand C, Groutas WC, Bannasch M, Meadows JM, Chang KO, 2018. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. Journal of Feline Medicine and Surgery 20, 378–392.
Pedersen NC, Perron M, Bannasch M, Montgomery E, Murakami E, Liepnieks M, Liu H, 2019. Efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. Journal of Feline Medicine and Surgery 21, 271–281.
Peiffer RL Jr, Wilcock BP, 1991. Histopathologic study of uveitis in cats: 139 cases (1978-1988). Journal of the American Veterinary Medical Association 198, 135–138.
Pesteanu-Somogyi LD, Radzai C, Pressler BM, 2006. Prevalence of feline infectious peritonitis in specific cat breeds. Journal of Feline Medicine and Surgery 8, 1–5.
Poland AM, Vennema H, Foley JE, Pedersen NC, 1996. Two related strains of feline infectious peritonitis virus isolated from immunocompromised cats infected with the feline enteric coronavirus. Journal of Clinical Microbiology 34, 3180–3184.
Regan A, Whitaker G, 2008. Utilization of DC-SIGN for entry of feline coronaviruses into host cells. Journal of Virology 82, 11992-11996.
Riemer F, Kuehner KA, Ritz S, Sauter-Louis C, Hartmann K, 2016. Clinical and laboratory features of cats with feline infectious peritonitis – a retrospective study of 231 confirmed cases (2000-2010). Journal of Feline Medicine and Surgery 18, 348–356.
Rohrbach BW, Legendre AM, Baldwin CA, Lein DH, Reed WM, Wilson RB, 2001. Epidemiology of feline infectious peritonitis among cats examined at veterinary medical teaching hospitals. Journal of the American Veterinary Medical Association 218, 1111–1115.
Rojko J, Hoover E, Quackenbush, S. Olsen RG, 1982. Reactivation of latent feline leukemia virus infection. Nature 298, 385–388.
Sheahan TP, Sims AC, Zhou S, Graham RL, Pruijssers AJ, Aostini, ML, Leist, SR, Schäfer, A, Dinnon, KH 3rd., Stevens, LJ et al., 2020. An orally bioavailable broad-spectrum antiviral inhibitions SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Science Translational Medicine. 12, eabb5883.
Spencer, SE, Knowles, T, Ramsey, IK. 2017. Pyrexia in cats. retrospective analysis of signalment, clinical investigations, diagnosis and influence of prior treatment in 106 referred cases. Journal of Feline Medicine and Surgery 19, 1123–1130.
Stella J, Croney C, Buffington T, 2013. Effects of stressors on the behavior and physiology of domestic cats. Applied Animal Behavior Science 143, 157-163.
Stranieri A, Giordano A, Bo S, Braghiroli C, Paltrnieri S, 2017. Frequency of electrophoretic changes consistent with feline infectious peritonitis in two different time periods (2004–2009 vs 2013–2014). Journal of Feline Medicine and Surgery 19, 880–887.
Takano T, Katoh Y, Doki T, Hohdatsu T, 2013. Effect of chloroquine on feline infectious peritonitis virus infection in vitro and in vivo. Antiviral Research. 99, 100–107.
Tasker S, 2018. Diagnosis of feline infectious peritonitis: Update on evidence supporting available tests. Journal of Feline Medicine and Surgery 20, 228–243.
Tekes G, Ehmann R, Boulant S, Stanifer ML, 2020. Development of feline ileum- and colon-derived organoids and their potential use to support feline coronavirus infection. Cells 9, 2085.
Terada Y, Matsui N, Noguchi K, Kuwata R, Shimoda H, Soma T, Mochizuki M, Maeda K, 2014. Emergence of pathogenic coronaviruses in cats by homologous recombination between feline and canine coronaviruses. PLoS One 9, e106534.
Van Hamme E, Dewerchin HL, Cornelissen E, Verhasselt B, Nauwynck HJ, 2008. Clathrin- and caveolae-independent entry of feline infectious peritonitis virus in monocytes depends on dynamin. Journal of General Virology 89, 2147–2156.
Vennema H, Poland A, Foley J, Pedersen NC, 1995. Feline infectious peritonitis viruses arise by mutation from endemic feline enteric coronaviruses. Virology 243, 150–157.
Vogel L, Van der Lubben M,, Te Lintelo EG, Bekker CPJ, Geerts T, Schuif LS, Grinwis GCM, Egberink HF, Rottier PJM, 2010. Pathogenic characteristics of persistent feline enteric coronavirus infection in cats. Veterinary Research 41, 71.
Vuong, W, Fischer C, Khan MB, van Belkum MJ, Lamer T, Willoughby, KD, Lu, J, Arutyenova, E, Joyce, MA, Saffran, HA et al., 2021. Improved SARS-CoV-2 Mpro inhibitors based on feline antiviral drug GC376: Structural enhancements, increased solubility, and micellar studies. European Journal of Medicinal Chemistry, 222, 113584.
Wang YT, Su BL, Hsieh LE, Chueh LL, 2013. An outbreak of feline infectious peritonitis in a Taiwanese shelter: Epidemiologic and molecular evidence for horizontal transmission of a novel type II feline coronavirus. Veterinary Research, 44, 57.
Ward JM, 1970. Morphogenesis of a virus in cats with experimental feline infectious peritonitis. Virology 41, 191–194.
Watanabe R, Eckstrand C, Liu H, Pedersen NC, 2018. Characterization of peritoneal cells from cats with experimentally-induced feline infectious peritonitis (FIP) using RNA-seq. Veterinary Research 49, 81.
Weiss RC, Scott FW, 1981. Antibody-mediated enhancement of disease in feline infectious peritonitis: comparisons with dengue hemorrhagic fever. Comparative Immunology, Microbiology and Infectious Diseases 4, 175-189.
Weiss RC, Cox NR, Martinez ML, 1993. Evaluation of free or liposome-encapsulated ribavirin for antiviral therapy of experimentally induced feline infectious peritonitis. Research in Veterinary Science 55, 162e72.
Wolfe, LG, Griesemer, RA, 1971. Feline infectious peritonitis: a review of gross and histopathologic lesions. Journal of the American Veterinary Medical Association 158, 987–993.
Worthing KA, Wigney DI, Dhand NK, Fawcett A, McDonagh P, Malik R, Norris JM, 2012. Risk factors for feline infectious peritonitis in Australian cats. Journal of Feline Medicine and Surgery 14, 405–412.
Yan VC, Muller FL, 2020. Advantages of the Parent Nucleoside GS-441524 over Remdesivir for Covid-19 Treatment. ACS Medicinal Chemistry Letters 11, 1361–1366
Yu J, Kimble B, Norris JM, Govendir M, 2020. Pharmacokinetic profile of oral administration of mefloquine to clinically normal cats: A preliminary in-vivo study of a potential treatment for feline infectious peritonitis (FIP). Animals 10, 1000.
Yuki M, Aoyama R, Nakagawa M, Hirano T, Naitoh E, Kainuma D, 2020. A Clinical Investigation on serum amyloid A concentration in client-owned healthy and diseased cats in a primary care animal hospital. Veterinary Sciences, 7, 45.
Ziółkowska N, Paździor-Czapula K, Lewczuk B, Mikulska-Skupień E, Przybylska-Gornowicz B, Kwiecińska K, Ziółkowski H, 2017. Feline infectious peritonitis: immunohistochemical features of ocular inflammation and the distribution of viral antigens in the structures of the eye. Veterinary Pathology, 54, 933-940.
Zook BC, King NW, Robinson RL, McCombs HL, 1968. Ultrastructural evidence for the viral etiology of feline infectious peritonitis. Veterinary Pathology 5, 91–95.
Hughes D, Howard G, Malik R, 2021. Treatment of FIP in cats with Remdesivir. Clinical review, 2021. The Veterinarian. https://www.turramurravet.com.au/wp-content/uploads/2021/07/FIP-Article_The-Veterinarian.pdf (Accessed 5 March 2022).
Anonymous. Thanks to Cats, One Promising Coronavirus Treatment is Already in Development-The GC376 story. 2021, https://anivive.com/coronavirus (Accessed 4 April 2022)
Those who have followed my career know that I have many interests in addition to infectious diseases of cats. However, I am best known for feline medicine and diseases that plague multi-cat environments. This interest in infectious diseases started in 1965 as a second-year veterinary student but evolved after I joined the faculty of the UC Davis School of Veterinary Medicine in 1972. My first appointment was to help win President Nixon’s war on cancer. This war emphasized potential viral causes of cancer, in particular retroviruses and human leukemias. This was my entry back into the world of feline leukemia virus (FeLV). Of course, my interest was more on FeLV infection as it applied to cats than any application to human cancers. It became rapidly apparent that FeLV infection was a serious panzootic (pandemic) of cats that had unknowingly spread from feral to pet cats in the preceding decades and would account for one-third of mortality in cats in the 1960s and 70s. Cat lovers quickly mobilized once the virus was discovered and started raising money to support FeLV research. The original SOCK was created by a group of amazing cat lovers led by Vince, Connie and Dorothy Campanile and friends. SOCK it to leukemia became the rallying cry of the group and I was privileged to join forces with them from their beginning to end. Thereafter, donations from cat lovers and not federal research funds provided the bulk of our research into FeLV infection at UC Davis. This research led to an understanding of how FeLV became a pandemic of pet cats, how it caused a wide range of diseases, and how it could be controlled. FeLV infection of pet cats was brought under control in the 1970’s and 1980’s through rapid diagnostic tests and vaccination. The conquest of FeLV infection was one of the highlights of veterinary research of the period, and perhaps one of the most important contributions of modern feline medicine in the 20th century. SOCK it to leukemia had ultimately worked itself out of existence with over $1M dollars raised towards the ultimate conquest of FeLV infection. FeLV infection still exists in nature, where it remains a problem for a small number of younger cats coming into foster/rescues and shelters from the field.
At the same time, another very deadly disease emerged. In 1963, veterinarians at Angell Memorial Animal Hospital in Boston first recorded feline infectious peritonitis (FIP). It was later found to be closely related to FeLV infection, and it was hoped that with FeLV control, it would largely disappear. This was not confirmed, and FIP soon replaced FeLV as the leading infectious cause of death in cats. As a result, the torch was passed from “SOCK it to leukemia” to “SOCK it to FIP.” This was also a natural progression for my research. FIP had been my first “love” since I helped investigate the first cases of FIP as a veterinary student at the University of California, Davis in 1965. My interest in FIP briefly took a back seat in the 1980s when I was working on HIV/AIDS and subsequently discovered feline immunodeficiency virus (FIV). FIP has become the main focus of my research for the past three decades.
I am pleased to have had the support of SOCK FIP over these later years. One of our greatest discoveries at UC Davis was how an innocuous and ubiquitous feline enteric coronavirus (FECV) ends up causing such a highly fatal disease as FIP. Our theory that the virus of FIP arose as an internal mutation of FECV was first met with great skepticism but is now universally accepted. The internal mutation theory has led to a much better understanding of the conditions under which FIP occurs and how the FIP virus causes disease. Unfortunately, no one, including us, was able to find a successful vaccine for FIP. This failure led to my interest in curing rather than preventing FIP using modern antiviral drugs, which I became familiar with during the HIV/AIDS pandemic. The capstone of my almost 50-year experience with FIP was the discovery of two antiviral drugs that could cure FIP. Thousands of cats from round the world have been cured of FIP with antiviral drugs researched at UC Davis over the last 3 years. Our discoveries at UC Davis could have been impossible without the significant long-term financial and moral support of SOCK FIP and cat owners who have donated money.
The discovery of a cure for FIP has once again brought SOCK FIP to a logical ending, just as the conquest of FeLV infection ended the need for the original SOCK. Although I am retired, I continue to work with cat owners and caregivers on how to use antiviral drugs to treat FIP and will maintain my relationship with SOCK FIP as a consultant on FIP treatment and a lifelong member. Admittedly, there is still research to be done with FIP, mainly in the areas of disease prevention. Hopefully, others will take up this and other areas of FIP research. The question now is how SOCK can best improve the health of our cats and kittens. SOCK FIP is in the process of evaluating a broader mission than just FIP. This mission may or may not involve fund raising for research and could be more informational. We welcome suggestions on how the long history of SOCK’s can be used to improve the health of our cats and kittens.
Origin of FIP exudates. Sweat in wet FIP comes from small vessels (venules) that line the surface of the abdominal and thoracic organs (visceral) and walls (parietal), mesentery / mediastinum, and omentum. The spaces around these vessels contain a specific type of macrophages that come from monocyte progenitors that constantly recirculate between the bloodstream, the interstitial spaces around the venules, the afferent lymph, the regional lymph nodes, and back into the bloodstream. Other sites of this recirculation are located in the meninges, brain ependyma, and uveal eye tract. A small proportion of these monocytes develop into immature macrophages (monocyte / macrophage) and eventually into resident macrophages. Macrophages are constantly looking for infections.
FIPV is caused by a mutation in feline enteric coronavirus (FECV) present in lymphoid tissues and lymph nodes in the lower intestine. The mutation changes FECV cell tropism from enterocytes to peritoneal-type macrophages. Monocytes / macrophages appear to be the first cell type to be infected. This infection causes more monocytes to leave the bloodstream and begin to turn into macrophages, which continue the cycle of infection. [2]. Monocytes / macrophages do not undergo programmed cell death as usually expected, but continue to mature into large virus-loaded macrophages. These large macrophages eventually undergo programmed cell death (apoptosis) and release large amounts of virus, which then infects new monocytes / macrophages. [1]. Infected monocytes / macrophages and macrophages produce several substances (cytokines) that mediate the intensity of inflammation (disease) and immunity (resistance). [1,2].
Inflammation associated with FIP leads to three types of changes in the venules. The first is loss of vascular wall integrity, micro-bleeding, and leakage of plasma protein rich in activated complement clotting and activation factors and other inflammatory proteins. The second type of damage involves thrombosis and blocking blood flow. The third injury occurs in more chronic cases and involves fibrosis (scarring) around the blood vessels. Variations in these three events determine the amount and composition of exudates according to the four Starling forces that determine the movement of fluids between the bloodstream and interstitial spaces. [3].
The classic effusion in wet FIP is mainly due to acute damage to the vessel walls and leakage of plasma into the interstitial spaces and finally into the body cavities. Protein that escapes into the interstitial spaces attracts additional fluids, which can be exacerbated by blocking venous blood flow and increasing capillary pressure. This type of effusion, known as exudate, also contains high levels of protein, which is involved in inflammation, immune responses and blood clotting.
This fluid also contains a large number of neutrophils, macrophages / monocytes, macrophages, eosinophils and a lower number of lymphocytes and red blood cells. This classic type of fluid has the consistency of egg white and forms weak clots containing a high amount of bilirubin. Bilirubin does not originate from liver disease, but rather from the destruction of red blood cells that escape into interstitial tissue cells and are taken up by monocytes / macrophages and macrophages. Red blood cells break down and hemoglobin is broken down into heme and globin. Globin is further metabolized to biliverdin (greenish color) and finally to bilirubin (yellowish color), which is then excreted by the liver. However, cats lack the enzymes used for conjugation and are therefore ineffective in removing bilirubin from the body. [4]. This leads to the accumulation of bilirubin in the bloodstream and gives the effusion a yellow tinge. The darker the yellow tint, the more bilirubin is in the effusion, the more severe the initiating inflammatory response and the more severe the resulting bilirubinemia, bilirubinuria and jaundice.
At the opposite extreme of the classic and more acute effusion in FIP are effusions that arise predominantly from chronic infections and blockage of venous blood flow and subsequent elevation of capillary pressure. High capillary pressure results in an effusion that more closely resembles interstitial fluid than plasma, has a lower protein content, is watery rather than viscous, is clear or slightly yellow in color, is not prone to clotting, and has a lower number of acute inflammatory cells such as neutrophils. There are also FIP effusions that fall between these extremes, depending on the relative degree of acute inflammation and chronic fibrosis. These transitional types of fluid are commonly referred to in the veterinary literature as modified transudate, but this is a misnomer. Modified transudate begins as a transudate and changes as it persists and causes mild inflammation. The low-protein, low-cell effusions of FIP arise as exudates rather than transudates and do not fit this description. A more accurate term is “modified exudate” or “variant exudative effusion.”
How long do sweats usually last in cats treated with GS-441524 or GC376? The presence of abdominal effusions often leads to a large dilation of the abdomen and is confirmed by palpation, hollow needle aspiration, X-ray or ultrasound. Cats with thoracic effusions are most often presented with severe shortness of breath and are confirmed by radiological examination and aspiration. Chest effusions are almost always removed to relieve shortness of breath and recur slowly compared to abdominal effusions. Therefore, abdominal effusions are usually not removed unless they are massive and do not interfere with respiration, as they are quickly replaced. Repeated drainage of abdominal effusions can also deplete proteins and cause harmful changes in fluid and electrolyte balance in severely ill cats.
Chest effusions disappear faster with GS-441524 treatment, with improved breathing within 24-72 hours and usually disappearing in less than 7 days. Abdominal effusions usually decrease significantly within 7-14 days and disappear within 21-28 days. The detection of exudates that persist after this time depends on their amount and method of detection. Small amounts of persistent fluid can only be detected by ultrasound.
Persistence of exudates during or after antiviral treatment. There are three basic reasons for the persistence of exudates. The first is the persistence of the infection and the resulting inflammation at a certain level, which can be caused by inappropriate treatment, poor medication or drug resistance. Inadequate treatment may be the result of incorrect dosing of the wrong drug or the acquisition of virus resistance to the drug. The second reason for fluid persistence is chronic venous damage and increased capillary pressure. This may be due to a low-grade infection or residual fibrosis from an infection that has been removed. The third reason for persistence is the existence of other diseases, which can also manifest as exudates. These include congenital heart disease, in particular cardiomyopathy, chronic liver disease (acquired or congenital), hypoproteinemia (acquired or congenital) and cancer. Congenital diseases causing effusions are more common in young cats, while acquired causes and cancer are more commonly diagnosed in older cats.
Diagnosis and treatment of persistent effusions. A thorough examination of the fluid, as described above, is a prerequisite for diagnosis and treatment. If the fluid is inflammatory or semi-inflammatory and the cell pellet is positive by PCR or IHC, the reason for the persistence of the infection must be determined. Was the antiviral treatment performed correctly, was the antiviral drug active and its concentration correct, was there evidence of acquired drug resistance? If the fluid is inflammatory and PCR and IHC are negative, what other diseases are possible? Low protein and non-inflammatory fluids that are negative for PCR and IHC indicate a diagnosis of residual small vessel fibrosis and / or other contributing causes such as heart disease, chronic liver disease, hypoproteinemia (bowel disease or kidneys). Some of the disorders causing this type of effusion may require an exploratory laparotomy with a thorough examination of the abdominal organs and a selective biopsy to determine the origin of the fluid. The treatment of persistent effusions will vary greatly depending on the end cause. Persistent effusions caused by residual small vessel fibrosis in cats cured of the infection often resolve after many weeks or months. Persistent discharges caused in whole or in part by other diseases require treatment for these diseases.
Identification and characteristics of persistent effusions. The presence of fluid after 4 weeks of GS treatment is unpleasant and is usually detected in several ways depending on the amount of fluid and its location. Large amounts of fluid are usually determined by the degree of abdominal dilation, palpation, X-ray and abdominal aspiration, while smaller amounts of fluid are best detected by ultrasound. Persistent pleural effusion is usually detected by X-rays or ultrasound. Overall, ultrasound is the most accurate means of detecting and semiquantitatively determining thoracic and abdominal effusions. Ultrasound can also be used in combination with thin needle aspiration to collect small and localized amounts of fluid.
The second step in examining persistent effusions is to analyze them based on color, protein content, white and red blood cell counts, and the types of white blood cells present. Fluids generated primarily by inflammation will have protein levels close to or equal to plasma and a large number of white blood cells (neutrophils, lymphocytes, monocytes / macrophages and large vacuolated macrophages). Fluids produced by increased capillary pressure are more similar to interstitial fluid with proteins closer to 2.0 g / dl and cell counts <200. The Rivalt test is often used to diagnose FIP-related effusions. However, this is not a specific test for FIP, but rather for inflammatory effusions. It is usually positive for FIP effusions that are high in protein and cells, but is often negative for very low protein and cell effusions. The effluents that are between these two types of effusions will be tested either positively or negatively, depending on where they are in the spectrum.
The third step is the analysis of exudates for the presence of FIP virus. This usually requires 5 to 25 ml or more of fluid. For fluids with a higher protein and cell count, a smaller amount may suffice, while for fluids with a low protein and cell count, a larger amount is required. The freshly collected sample should be centrifuged and the cell pellet analyzed for the presence of viral RNA by PCR or cytocentrifuged for immunohistochemistry (IHC). The PCR test should be for FIPV 7b RNA and not for specific FIPV mutations, as the mutation test does not have sufficient sensitivity and does not provide any diagnostic benefits [5]. Samples that are positive by PCR or IHC provide definitive evidence of FIP. However, up to 30 % samples from known cases of FIP may have a false negative test either due to an inappropriate sample and its preparation, or because the RNA level of the FIP virus is below the level of detection. It is also true that the less inflammatory the fluid, the lower the virus levels. Therefore, effusions with lower protein and white blood cell levels are more likely to be tested negative because viral RNA is below the detection limit of the test.
References
[1] Watanabe R, Eckstrand C, Liu H, Pedersen NC. Characterization of peritoneal cells from cats with experimentally-induced feline infectious peritonitis (FIP) using RNA-seq. Vet Res. 2018 49 (1): 81. doi: 10.1186 / s13567-018-0578-y.
[2]. Kipar A, Meli ML, Failing K, Euler T, Gomes-Keller MA, Schwartz D, Lutz H, Reinacher M. Natural feline coronavirus infection: differences in cytokine patterns in association with the outcome of infection. Vet Immunol Immunopathol. 2006 Aug 15; 112 (3-4): 141-55. doi: 10.1016 / j.vetimm.2006.02.004. Epub
[4]. Court MH. Feline drug metabolism and disposition: pharmacokinetic evidence for species differences and molecular mechanisms. Vet Clin North Am Small Anim Pract. 2013; 43 (5): 10391054. doi: 10.1016 / j.cvsm.2013.05.002
[5]. Barker, EN, Stranieri, A, Helps, CR. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet Res 2017; 48: 60.
ABSTRACT: Acute phase proteins (APP) are proteins synthesized and released mainly by hepatocytes when cells are damaged or invaded by microorganisms. This article reviews the use of APPs in feline diseases, identifies their utility in the clinical setting, and analyzes 55 published papers. Serum amyloid A (SAA), alpha-1 acid glycoprotein (AGP), and haptoglobin are markers that the authors consider useful in monitoring the acute inflammatory response in cats. Although measurement of APP is still not routinely used in veterinary medicine, together with clinical signs and other blood parameters, they are of clinical interest and applicable in diseases such as feline infectious peritonitis, pancreatitis, renal failure, retroviral and calicivirus infections. Although there are commercially available kits for measuring feline APP, standardization of assays aimed at technical simplicity, greater species specificity, and lower associated costs will enable routine use in feline practice, as is done in the human field. keywords: inflammation, acute phase proteins, cat.
Introduction
Acute phase response (APR) is an early non-specific systemic innate immune response to a local or systemic stimulus that helps treat and restore homeostasis and minimize tissue damage when an organism is affected by trauma, infection, stress, surgery, neoplasia, or inflammation (GRUYS et al. , 2005; CRAY et al., 2009; ECKERSALL AND BELL, 2010). In this reaction, we observe several different systemic effects: fever, leukocytosis, hormonal changes - mainly cortisol and thyroxine concentrations, with secondary catabolic status and serum muscle, iron and zinc depletion (CERÓN et al. 2005, JAVARD et al. 2017). Cytokines IL-1β, TNF-α, and especially IL-6, and approximately 90 minutes after injury, increase protein synthesis in hepatocytes, lymph nodes, tonsils, and spleen, as well as blood leukocytes. These newly formed proteins are called acute phase proteins (APPs) (TIZARD, 2013b).
Acute-phase proteins
APP concentrations may increase (APP positive) or decrease (APP negative) in response to inflammation (PALTRINIERI et al., 2008) (JOHNSTON & TOBIAS, 2018). They can activate leukocytosis and complement, cause protease inhibition, lead to blood clotting and opsonization - a defense mechanism that leads to the elimination of infectious agents, tissue regeneration and restoration of health (CRAY et al., 2009). APP can have two functions, pro- and / or anti-inflammatory, which must be fine-tuned to promote homeostasis (HOCHEPIED et al., 2003).
According to the size and duration of the reaction following the stimulus, three main groups of APP are distinguished (MURATA et al., 2004; PETERSEN et al., 2004; CERÓN et al.). Positive APP can be divided into two groups: the first group includes APP with an increase of 10 up to 1000-fold in humans or 10- to 100-fold in domestic animals in the presence of inflammation - e.g. c-reactive protein (CRP) and serum amyloid A (SAA). The second group are APPs, which increase 2 to 10-fold in an inflammatory response - e.g. haptoglobin and alpha-globulins. The last group included negative APP, in which the concentration decreases in response to inflammation - e.g. albumin (KANN et al., 2012).
Acute phase positive proteins
Positive APPs are glycoproteins whose serum concentrations, when stimulated by pro-inflammatory cytokines, increase by 25 % during the disease process and are released into the bloodstream. These concentrations can be measured and used in diagnosis, prognosis, monitoring of response to treatment, as well as general health screening. They can also be considered as quantitative biomarkers of the disease, highly sensitive to inflammation but not very specific, as an increase in APP can also occur in non-inflammatory diseases (CERÓN et al., 2005; ECKERSALL and BELL, 2010).
Positive APPs respond to cytokines differently, and these groups fall into two main classes. Type 1 APP, which includes AGP, complement component 3, SAA, CRP, haptoglobin and hemopexin, is regulated by IL-1, IL-6 and TNF-α as well as glucocorticoids. Type 2, which includes three fibrinogen chains (α-, β- and γ-fibrinogen) and various inhibitory proteases, is regulated by cytokines IL-6 and glucocorticoids (BAUMANN et al., 1990; BAUMANN & GAULDIE, 1994).
In cats, the most important APP is SAA (Serum Amyloid A) or alpha-1-acid glycoprotein (AGP). The level of SAA in the blood can indicate inflammatory conditions such as feline infectious peritonitis (FIP) and other infectious diseases such as calicivirus infection, chlamydiosis, leukemia and infectious immunodeficiency, as it increases 10- to 50-fold (TIZARD, 2013b). SAA can also be elevated in other diseases such as diabetes mellitus and cancer. Haptoglobin is usually increased 2- to 10-fold and is particularly high in FIP (TIZARD, 2013b). Table 1 summarizes the individual positive APPs in the context of feline disease.
Acute phase negative proteins
The most significant negative APP is albumin, whose blood concentration decreases during APR due to amino acid aberrations towards the synthesis of positive APPs (CRAY et al., 2009; PALTRINIERI, 2007a). Other negative APPs are transferrin, transthyretin, retinol ligand, and cortisol binding protein, proteins involved in vitamin and hormone transport (JAIN et al., 2011).
Acute phase proteins in cat disease
Unlike cytokines, which are small in size and rapidly filtered by the kidney, acute phase proteins have a higher molecular weight (greater than 45 kDa) and consequently remain in plasma for longer (SALGADO et al., 2011).
APP levels can only indicate inflammation, and consequently their concentrations can help diagnose and monitor the disease. APP can help detect subclinical inflammation, distinguish acute from chronic disease, and predict its course (VILHENA et al, 2018; JAVARD et al., 2017). Because APRs begin before specific immunological changes occur, they can be used as an early marker of disease before leukogram changes occur, with their magnitude related to disease severity (PETERSEN et al., 2004; CÉRON et al., 2005; VILHENA et al., 2005). , 2018). For this reason, disease monitoring can be considered one of the most interesting and promising applications of APP.
APP levels along with clinical signs and blood tests have been evaluated in a variety of animal diseases (ie, FIP, canine inflammatory disease, leishmaniasis, ehrlichiosis, and canine pyometra) and have been shown to be useful in diagnosis, response to treatment, and prognosis (ECKERSALL et al. ), 2001; MARTINEZ-SUBIELA et al., 2005; SHIMADA et al., 2002; JERGENS et al., 2003; GIORDANO et al., 2004; PETERSEN et al., 2004; DABROWSKI et al., 2009; VILHENA et al., 2018).
To obtain complete information on APR, one major and one moderate positive as well as one negative APP should be evaluated simultaneously (CERÓN et al., 2008). High concentrations of major APP are usually associated with infectious diseases, usually systemic bacterial infection or immune-mediated disease (CERÓN et al., 2008; TROÌA et al., 2017). Although APPs should be analyzed along with white blood cell and neutrophil counts, they are most sensitive in the early detection of inflammation and infection (CERÓN et al., 2008; ALVES et al., 2010). However, the specificity of these proteins is low in determining the cause of the process, and also increases in physiological conditions such as pregnancy (PALTRINIERI et al., 2008).
APP
The disease
SAA
FIP Induced inflammation and surgery Various diseases (pancreatitis, renal failure, FLUTD, tumors, diabetes mellitus; kidney disease, injury, etc.) Sepsis FeLV; hemotropic mycoplasma infections Hepatozoonfelis and Babesia vogeli infection Dirofilariaimmitis FIV cats treated with recombinant feline interferon
AGP
Chlamydophila psittaci infection; Pancreatitis and pancreatic tumors FIP Lymphoma and other tumors Induced inflammation and surgery FIV cats treated with recombinant feline interferon Abscesses, pyothorax, adipose tissue necrosis Various diseases (FLUTD, tumors, diabetes mellitus, kidney diseases, injuries, etc.)
Haptoglobin
FIP Induced inflammation and surgery Abscesses, pyothorax, adipose tissue necrosis Various diseases (FLUTD, tumors, diabetes mellitus, kidney diseases, injuries, etc.) Hepatozoonfelis and Babesia vogeli infection FeLV, hemotropic mycoplasmas Dirofilariaimmitis
CRP
FIV cats treated with recombinant feline interferon Induced inflammation and surgery
Figure 1 shows the expected behavior of acute phase positive proteins based on revised studies. AGP, SAA and haptoglobin have been identified as useful indicators for monitoring the acute inflammatory response in cats (WINKEL et al., 2015; PALTRINIERI et al., 2007a, b; KAJIKAWA et al., 1999). APPs in cats were first identified after comparative measurements in the serum of clinically normal and diseased animals, in experimentally induced inflammation studies, and in postoperative studies (KAJIKAWA et al., 1999). The concentration of SAA reportedly increased first, followed by an increase in AGP and haptoglobin, in contrast to a less pronounced increase in CRP (KAJIKAWA et al., 1999). One study showed that CRP behaves similarly to SAA and AGP in cat inflammation (LEAL et al., 2014).
Serum Amyloid A
SAA is one of the major APPs in several species, important in both humans and cats (KAJIKAWA et al., 1999). It modulates the immune response by attracting inflammatory cells to tissues and leading to the production of multiple inflammatory cytokines (GRUYS et al., 2005; TIZARD, 2013a). Its concentration can increase more than 1,000 times in an inflammatory condition, which we then understand as inflammation (TAMAMOTO et al., 2013). However, such an increase can be observed in both non-inflammatory and inflammatory diseases and neoplasms (TAMAMOTO et al., 2013). According to a study in cats that underwent surgery, SAA levels begin to increase approximately 3 to 6 hours, peaking 21 to 24 hours after surgery (SASAKI et al., 2003).
Figure 1 - Idealized behavior of acute phase proteins in cats after inflammatory stimuli. The values representing the changes cannot be considered absolute. Increase in serum amyloid A (SAA) 3 to 6 h after challenge, peak at 21 to 24 h, peak size 10 to 50 times its basal plasma concentration. Alpha 1 acid glycoprotein (AGP) increases 8 h after challenge, peak at 36 h, size at peak time 2 to 10 times its baseline plasma concentration. Haptoglobulin (Hp) increase 24 h after challenge, peak 36 to 48 h, peak size 2 to 10 times its basal plasma concentration. C-reactive protein (CRP) increased 8 h after challenge, peak at 36 h, peak size 1.5 times its basal values.
Alpha 1-acid glycoprotein
Alpha 1-acid glycoprotein (AGP) is an acute phase-reactive protein found in the serum mucoid portion of serum (SELTING et al., 2000; WINKEL et al., 2015). Like most positive APPs, AGP is a glycoprotein synthesized predominantly by hepatocytes in APR and released into the bloodstream (CÉRON et al., 2005).
AGP can be used to monitor early interferon treatment in cats infected with feline immunodeficiency virus (FIV) (GIL et al., 2014). AGP as well as haptoglobin (Hp) are increased in anemic cats suffering from pyothorax, abscesses or fat necrosis (OTTENJANN et al., 2006).
Changes in AGP in feline neoplasia do not appear to be consistent across studies. Some of them do not describe any changes in cats with lymphoma (CORREA et al., 2001). Others point to an increase in both AGP and SAA in cats with sarcomas, carcinomas, or other round cell tumors (SELTING et al., 2000; TAMAMOTO et al., 2013; MEACHEN et al., 2015; HAZUCHOVA et al., 2017).
AGP is important as an indicator test for FIP, which is used specifically in Europe (CECILIANI et al., 2004). GIORI et al. examined the specificity and sensitivity of several tests in 12 cats, with 33.33 % cats being FIP negative based on histopathology and immunohistochemistry and 66.66 % cats being FIP positive confirmed by histopathology and immunohistochemistry. This author concludes that immunohistochemistry must always be performed to confirm FIP, but high concentrations of AGP can help support the diagnosis of FIP if immunohistochemistry cannot be performed and histopathology is not convincing.
Haptoglobin
Haptoglobin (Hp) is one of the most important acute phase proteins in cattle, sheep, goats, horses and cats (TIZARD, 2013a), synthesized mainly by hepatocytes but also by other tissues such as skin, lungs and kidneys (JAIN et al, 2011 ). Hp binds to iron molecules and makes them inaccessible to invasive bacteria, thereby inhibiting bacterial proliferation and invasion. Subsequently, it also binds to free hemoglobin, thus preventing its oxidation with lipids and proteins (TIZARD, 2013a), which justifies a reduction in Hp in case of hemolysis.
In cats, Hp usually increases 2- to 10-fold in inflammatory conditions, and is particularly high in FIP (TIZARD, 2013a). However, both Hp and SAA did not provide sufficient support to distinguish FIP from other causes of effusion compared to AGP (HAZUCHOVÁ et al., 2017).
Measurement APP
The serum is composed of a large number of individual proteins in which the detection of changes in its fractions can provide important diagnostic information (ECKERSALL, 2008).
Ideally, measurement of all serum proteins should be available so that they can be used as a diagnostic tool in relation to inflammatory diseases. Currently, APPs (Table 2) can be determined by enzyme-linked immunosorbent assay (ELISA), radioimmunoassay, nephelometry, immunoturbidimetry (IT), Western blot, and messenger ribonucleic acid (mRNA) analysis (CÉRON et al., 2005; PALTRINIERI et al., 2008; SCHREIBER et al., 1989). Although some human APP tests have been automated for veterinary medicine, species-specific tests are still limited. Cross-species differences in APP and the limited availability of cross-reactive agents have so far contributed to the low routine level of APP determination in veterinary laboratories, especially in cats. Regardless, the technology is evolving and routine monitoring of clinically relevant APPs in cats can be expected in the near future.
Conclusion
Acute phase proteins in cats are biomarkers suitable for monitoring inflammation, along with other clinical and laboratory findings that are useful in diagnosing subclinical changes, monitoring the development and effect of the disease in the body, as well as in evaluating the response to treatment.
In cats, SAA APP, which is most pronounced in response to inflammation, is followed by AGP and haptoglobin, in contrast to CRP, which is used in other species.
Although there are commercially available kits for determining feline APPs, standardization of tests for technical simplicity, higher species specificity with lower associated costs will allow routine use in feline practice, as is done in human medicine.
Analyzes
Pros
Cons
Radioimmunoassay
24 to 48 hours to obtain results, specific operator skills required
ELISA
Commercially available species-specific kits
Lack of automation, expensive, some "between-run" inaccuracy
Immunoturbidimetry
30 minutes to obtain results, customizable with a biochemical analyzer
Western Blot
Long time for immunoblot processing
Nephelometric immunoassays
They depend on the cross-reactivity of the increased antiserum
Table 2 - Advantages and disadvantages of possible APP measurement techniques.
Appendix: APP and their position in the electrophoretogram
Although there are tests directly for a specific APP, it is useful to know in which region the electrophoretograms are located.
Electrophoretogram demonstration (Serum protein electrophoresis output)
Serum protein
Electrophoretic region
α1-acid glycoprotein
α1 (alpha-1)
Serum Amyloid A
α (alpha)
Haptoglobin
α2 (alpha-2)
Ceruloplasmin
α2 (alpha-2)
Transferrin
β1 (beta-1)
C-reactive protein
γ (gamma)
Position of serum proteins in electrophoretogram
References
ALVES, AE et al. Leucogram and serum acute phase protein concentrations in queens submitted to conventional or videolaparoscopic ovariectomy. Arquivo Brasileiro de Medicina Veterina- ria e Zootecnia, v.62, n.1, p.86-91, 2010. Available from:. Accessed: Oct. 10, 2018. doi: 10.1590 / S0102-09352010000100012.
BAUMANN, H. & GAULDIE, J. The acute phase response. Immunol Today, v.15, n.2, p.74-80, 1994. Available from: https://doi.org/10.1016/0167-5699(94)90137-6. Accessed: Aug. 21, 2018. doi: 10.1016 / 0167-5699 (94) 90137-6.
BAUMANN, H. et al. Distinct regulation of the interleukin-1 and interleukin-6 response elements of the rat haptoglobin gene in rat and human hepatoma cells. Molecular and Cellular Biology, v.10, n.11, p.5967–5976, 1990. Available from: Accessed: Aug. 21, 2018. doi: 10.1128 / MCB.10.11.5967.
BENCE, L. et al. An immunoturbidimetric assay for rapid quantitative measurement of feline alpha-1-acid glycoprotein in serum and peritoneal fluid. Veterinary Clinical Pathology, v.34, n.4, p335-341, 2005. Available from:. Accessed: Jan. 13, 2019. doi: 10.1111 / j.1939-165X.2005.tb00058.x.
CALLAHAN, G. & YATES, R. Veterinary Clinical Laboratory Immunology. In Warren, A. Basic Veterinary Immunology, pp. 295-317, 2014. Boulder, Colorado: University Press of Colorado.
CECILIANI, F. et al. Decreased sialylation of the acute phase protein α1-acid glycoprotein in feline infectious peritonitis (FIP). Veterinary Immunology and Immunopathology, v.99, n.3- 4, p.229-236, 2004. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j. vetimm.2004.02.003.
CERON, J. et al. Acute phase proteins in dogs and cats: current knowledge and future perspectives. Veterinary Clinical
Pathology, v.34, n.2, p.85-99, 2005. Available from:. Accessed: Aug. 20, 2018. doi: 10.1111 / j.1939-165X.2005.tb00019.x.
CERÓN, JJ A seven-point plan for acute phase protein interpretation in companion animals. Veterinary Journal, v.177, n.1, p.6-7, 2008. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / j. tvjl.2007.12.001.
CORREA, SS et al. Serum alpha 1-acid glycoprotein concentration in cats with lymphoma. Journal of the American Animal Hospital Association, v.37, n.2, p.153-158, 2001. Available from: https://doi.org/10.5326/15473317-37-2-153. Accessed: Aug. 24, 2018. doi: 10.5326 / 15473317-37-2-153.
CRAY, C. et al. AcutePhase Response in Animals: A Review. Comparative Medicine, v.59, n.6, p.517–526, 2009. Available from:. Accessed: Aug. 21, 2018.
DABROWSKI, R. et al. Usefulness of C-reactive protein, serum amyloid A component and haptoglobin determinations in bitches with pyometra for monitoring early postovariohysterectomy complications. Theriogenology, v.72, n.4, p.471–476, 2009. Available from:. Accessed: Aug. 23, 2018. doi: 10.1016 / j.theriogenology.2009.03.017.
DUTHIE, S. et al. Value of α1-acid glycoprotein in the diagnosis of feline infectious peritonitis. The Veterinary Record, v.141, n.12, p.299–303, 1997. Available from:. Accessed: Aug. 11, 2018. doi: 10.1136 / vr.141.12.299.
ECKERSALL, P. Proteins, Proteomics, and the Dysproteinemias. In Kaneko, J., Harvey, J. & Bruss, M. In Clinical Biochemistry of Domestic Animals. 6th ed. USA: Elsevier, 2008, Chap. 5, pp.117-155.
ECKERSALL, PD & BELL, R. Acute phase proteins: Biomarkers of infection and inflammation in veterinary medicine. The Veterinary Journal, v.185, n.1, p.23-27, 2010. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / j.tvjl.2010.04.009.
ECKERSALL, PD et al. Acute phase protein response in an experimental model of ovine caseous lymphadenitis. BMC Veterinary Research, v.19, p.3-35, 2007. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2010.04.009.
ECKERSALL, PD et al. Acute phase proteins in serum and milk from dairy cows with clinical mastitis. Veterinary Record, v.148, n.2, p.35–41, 2001. Available from:. Accessed: Aug. 22, 2018. doi: 10.1136 / vr.148.2.35.
GIL, S. et al. Oral recombinant feline interferon-omega as an alternative immune modulation therapy in FIV positive cats: Clinical and laboratory evaluation. Research in Veterinary Science, v.96, n.1, p.79–85, 2014. Available from:. Accessed: Oct. 10, 2018. doi: 10.1016 / j.rvsc.2013.11.007.
GIORDANO, A. et al. Changes in some acute phase protein and immunoglobulin concentrations in cats affected by feline infectious peritonitis or exposed to feline coronavirus infection. The Veterinary Journal, v.167, n.1, p.38-44, 2004. Available from: https://doi.org/10.1016/S1090-0233(03)00055-8. Accessed: Aug. 9, 2018. doi: 10.1016 / S1090-0233 (03) 00055-8.
GIORI, L. et al. Performances of different diagnostic tests for feline infectious peritonitis in challenging clinical cases. Journal of Small Animal Practice, v.52, n.3, p.152-157, 2011. Available from: https://doi.org/10.1111/j.1748-5827.2011.01042.x. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1748-5827.2011.01042.x.
GRUYS, E. et al. Acute phase reaction and acute phase proteins. Journal of Zhejiang University. Science B, v.6, n.11, p.1045- 1056, 2005. Available from:. Accessed: Aug. 21, 2018. doi: 10.1631 / jzus.2005.B1045.
HAZUCHOVA, K. et al. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. Journal of Feline Medicine and Surgery, v.19, n.8, p.809-816, 2017. Available from: https://doi.org/10.1177/1098612X16658925. Accessed: Aug. 11, 2018. doi: 10.1177 / 1098612X16658925.
HOCHEPIED, T. et al. α1-Acid glycoprotein: an acute phase protein with inflammatory and immunomodulating properties. Cytokine Growth Factor Rev, v.14, n.1, p.25–34, 2003. Available from: https://doi.org/10.1016/S1359-6101(02)00054-0. Accessed: Aug. 21, 2018. doi: 10.1016 / S1359-6101 (02) 00054-0.
JACOBSEN, S. et al. Evaluation of a commercially available human serum amyloid A (SAA) turbidometric immunoassay for determination of equine SAA concentrations. Veterinary Journal, v.172, n.2, p.315–319, 2006. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2005.04.021.
JAIN, S. et al. Acute-phase proteins: As diagnostic tool. Journal of Pharmacy and Bioallied Sciences, v.3 v.1, p.118–127, 2011. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3053509/. Accessed: Aug. 21, 2018. doi: 10.4103 / 0975-7406.76489.
JAVARD R. et al. Acute phase proteins and iron status in cats with chronic kidney Disease. Journal of Veterinary Internal Medicine, v.31, n.2, p.457-464, 2017. Available from:. Accessed: Oct. 10, 2018. doi: 10.1111 / jvim.14661.
JERGENS, AE et al. A scoring index for disease activity in canine inflammatory bowel disease. Journal of Veterinary Internal Medicine, v.17, n.3, p.291–297, 2003. Available from:. Accessed: Aug. 22, 2018. doi: 10.1111 / j.1939-1676.2003.tb02450.x.
KAJIKAWA, T. et al. Changes in concentrations of serum amyloid A protein, alpha 1-acid glycoprotein, haptoglobin, and C-reactive protein in feline sera due to induced inflammation and surgery. Veterinary Immunology and Immunopathology, v.68, n.1, p. 91-98, 1999. Available from: Accessed: Aug. 10, 2018. doi: 10.1016/S0165-2427(99)00012-4.
KANN, R. et al. Acute phase proteins in healthy and sick cats. Research in Veterinay Science, v.93, n.2. p.649-654, 2012. Available from: https://doi.org/10.1016/j.rvsc.2011.11.007. Accessed: Aug. 20, 2018. doi: 10.1016 / j.rvsc.2011.11.007.
KURIBAYASHI, T. et al. Alpha 1-acid glycoprotein (AAG) levels in healthy and pregnant beagle dogs. Experimental Animals, v.52, n. 5, p.377–381, 2003. Available from:. Accessed: Jan. 13, 2019. doi: 10.1538 / expanim.52.377.
LEAL, R. et al. Monitoring acute phase proteins in retrovirus infected cats undergoing feline interferon-ω therapy. Journal of Small Animal Practice, v.55, n.1, p.39-45, 2014. Available from: https://doi.org/10.1111/jsap.12160. Accessed: Jan. 6, 2019. doi: 10.1111 / jsap.12160.
MARTÍNEZ-SUBIELA, S. et al. Analytical validation of commercial techniques for haptoglobin determination, C reactive protein and amiloid A series in canines [Analytical validation of commercial techniques for haptoglobin, C reactive protein and serum amyloid A determinations in dogs]. Archivos de Medicina Veterinaria, v.37, n.1, 2005. Available from:. Accessed: Jan. 13, 2019. doi: 10.4067 / S0301-732X2005000100009.
MEACHEM, MD et al. A comparative proteomic study of plasma in feline pancreatitis and pancreatic carcinoma using 2-dimensional gel electrophoresis to identify diagnostic biomarkers: A pilot study. Canadian Journal of Veterinary Research, v.79, n.3, p.184-189, 2015. Available from:. Accessed: Oct. 10, 2018.
MURATA, H. et al. Current research on acute phase proteins in veterinary diagnosis: An overview. The Veterinary Journal, v.168, n.1, p.28–40, 2004. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / S1090-0233 (03) 00119-9.
OTTENJANN, M. et al. Characterization of the anemia of inflammatory disease in cats with abscesses, pyothorax, or fat necrosis. Journal of Veterinary Internal Medicine, v.2, n.5, p. 1143-1150, 2006. Available from:. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1939-1676.2006.tb00713.x.
PALTRINIERI, S. Early biomarkers of inflammation in dogs and cats: The acute phase protein. Veterinary Research Communications, v.31, n.1, p.125-129, 2007a. Available from: . Accessed: Aug. 21, 2018. doi: 10.1007 / s11259-007-0107-3.
PALTRINIERI, S. et al. Serum alpha1-acid glycoprotein (AGP) concentration in non-symptomatic cats with feline coronavirus (FCoV) infection. Journal of Feline Medicine and Surgery, v.9, n.4, p.271-277, 2007b. Available from:. Accessed: Aug. 11, 2018. doi: 10.1016 / j. jfms.2007.01.002.
PALTRINIERI, S. The feline acute phase reaction. Review. The Veterinary Journal, v.111, n.1, p.26-35, 2008. Available from: https://doi.org/10.1016/j.tvjl.2007.06.005. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2007.06.005.
PETERSEN, H. et al. Application of acute phase protein measurements in veterinary clinical chemistry. Veterinary Research, v.35, n.2, p.163–187, 2004. Available from:. Accessed: Aug. 20, 2018. doi: 10.1051 / vetres: 2004002.
SALGADO, FJ, et al. (2011). Acute phase proteins as biomarkers of disease: from Bench to Clinical Practice. In Veas, F. Acute Phase Proteins as Early Non-Specific Biomarkers of Human and Veterinary Diseases. Rijeka, Croatia: InTech. Available from: http://www.documentation.ird.fr/hor/fdi:010060045. Accessed: Aug. 21, 2018. doi: 10.5772 / 1045.
SASAKI, K. et al. Evaluation of feline serum amyloid A (SAA) as an inflammatory marker. Journal of Veterinary Medical Science, v.65, n.4, p.545-8, 2003. Available from:. Accessed: Aug. 10, 2018.
SCHREIBER, G. et al. The acute phase response in the rodent. Annals of the New York Academy of Science, v.557, p.61–85, 1989. Available from:. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1749- 6632.1989.tb24000.x.
SELTING, K. et al. Serum alpha 1-acid glycoprotein concentrations in healthy and tumor-bearing cats. Journal of Veterinary Internal Medicine, v.14, n.5, p.503-506, 2000. Available from:. Accessed: Aug. 9, 2018. doi: 10.1111 / j.1939-1676.2000.tb02267.x.
SHIMADA, T. et al. Monitoring C-reactive protein in beagle dogs experimentally inoculated with Ehrlichiacanis. Veterinary Research Communications, v.26, n.3, p.171–177, 2002. Available from:. Accessed: Aug. 22, 2018. doi: 10.1023 / A: 1015290903332.
SILVESTRE-FERREIRA, AC et al. Serum acute phase proteins in Dirofilariaimmitis and Wolbachia seropositive cats. Journal of Feline Medicine and Surgery, v.19, n.6, p.693–696, 2017. Available from: https://doi.org/10.1177/1098612X15625435. Accessed: Sep. 16, 2018. doi: 10.1177 / 1098612X15625435.
TAMAMOTO, T. et al. Serum amyloid A as a prognostic marker in cats with various diseases. Journal of Veterinary Diagnostic Investigation, v.25, n.3, p.428–432, 2013. Available from:. Accessed: Jan. 27, 2019.
TECLES, F. et al. Validation of a commercially available human immunoturbidimetric assay for haptoglobin determination in canine serum samples. Veterinary Research Communications, v.31, n.1, p.23–36, 2007. Available from:. Accessed: Jan. 13, 2019. doi: 10.1007 / s11259-006-3397-y.
TERWEE, J. et al. Characterization of the systemic disease and ocular signs induced by experimental infection with Chlamydia psittaci in cats. Veterinary Microbiology, v.59, 259-281, 1998. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / S0378-1135 (97) 00185-5.
TIZARD, I. Innate immunity: proinflammatory and antimicrobial mediators / systemic responses to inflammation. In Veterinary Immunology. 9.ed. St. Louis, Missouri: Saunders, Elsevier, 2013a. Chap. 6, pp.52-58.
TIZARD, I. Innate immunity: proinflammatory and Atimicrobial mediators / systemic responses to Inflammation. In Veterinary Immunology. 9.ed. St. Louis, Missouri: Saunders, Elsevier, 2013b. Chap. 4, pp.31-40.
TROÌA, R. et al. Serum amyloid A in the diagnosis of feline sepsis. Journal of Veterinary Diagnostic Investigation, v.29, n.6, p.856-859, 2017. Available from:. Accessed: Aug. 11, 2018. doi: 10.1177 / 1040638717722815.
VILHENA, H. et al. Acute phase proteins response in cats naturally infected by hemotropic mycoplasmas. Comparative Immunology, Microbiology & Infectious Diseases, v.56, p.1-5, 2018. Available from: https://doi.org/10.1016/j.cimid.2017.11.001. Accessed: Aug. 11, 2018. doi: 10.1016 / j.cimid.2017.11.001.
VILHENA, H. et al. Acute phase proteins response in cats naturally infected with Hepatozoonfelis and Babesia vogeli. Veterinary Clinical Pathology, v.48, n.1, p.72-76, 2017. Available from: https://doi.org/10.1111/vcp.12451. Accessed: Aug. 10, 2018. doi: 10.1111 / vcp.12451.
WEIDMEYER, C. & SOLTER, P. Validation of human haptoglobin immunoturbidimetric detection of haptoglobin in equine and canine serum and plasma. Veterinary Clinical Pathology, v.24, n.4, p.141–146, 1996. Available from:. Accessed: Jan. 13, 2019. doi: 10.1111 / j.1939-165X.1996.tb00988.x.
WHICHER, T. et al. Immunonephelometric and immunoturbidimetric assays for proteins. Critical Reviews in Clinical Laboratory Sciences, v.18, n.3, p.213–260, 1983. Available from: https://doi.org/10.3109/10408368209085072. Accessed: Aug. 13, 2019. doi: 10.3109 / 10408368209085072.
WINKEL, V. et al. Serum α-1 acid glycoprotein and serum amyloid A concentrations in cats receiving antineoplastic treatment for lymphoma. American Journal Veterinary Research, n.76, v.11, p.983-988, 2015. Available from:. Accessed: Aug. 22, 2018. doi: 10.2460 / ajvr.76.11.983.
Abbreviations: SC - subcutaneous IV - intravenous IM - to the muscle PO - per os - orally SID - once a day BID - 2x this q24h - once every 24 hours q12h - once in 12 hours
Introduction
Antiviral resistance is well documented in diseases such as HIV / AIDS and hepatitis C. In some cases, this resistance is present in the infecting virus, but is more often due to long-term drug exposure. Resistance to GC376 [1] and GS-441524 [2] has also been documented in cats with naturally acquired FIP. Resistance develops based on mutations in regions of the viral genome that contain targets for the antiviral drug. For example, several amino acid changes (N25S, A252S or K260N) were detected in the GIP376-resistant FIPV isolate (3CLpro). [3]. A change in N25S in 3CLpro was found to cause a 1.68-fold increase in 50 % GC376 inhibitory concentration in tissue cultures [3]. Resistance to GC376, although recognized in initial field trials, has not yet been described. GC376 is less popular in the treatment of FIP and is not recommended for cats with ocular or neurological FIP. [1].
Natural resistance to GS-441524 was observed in one of 31 cats treated for naturally occurring FIP [2]. One of the 31 cats in the original GS-441524 field study also appeared to be resistant, as viral RNA levels did not decrease throughout the treatment period and the symptoms of the disease did not abate. Although this virus has not been studied, resistance to GS-5734 (Remdesivir), a prodrug of GS-441524, has been established in tissue culture by amino acid mutations in RNA polymerase and corrective exonuclease. [4].
Resistance to GS-441524 has been confirmed in a number of cats that have been treated for FIP with GS-441524 in the last 3 years, especially among cats with neurological FIP [5]. Resistance to GS441524 is usually partial and higher doses often cure the infection or significantly reduce the symptoms of the disease during treatment. Interestingly, resistance to GS-441524 has also been found in patients with Covid19 treated with Remdesivir [12]. An immunocompromised patient developed a prolonged course of SARS-CoV-2 infection. Remdesivirus treatment initially alleviated symptoms and significantly reduced virus levels, but the disease returned with a large increase in virus replication. Whole genome sequencing identified an E802D mutation in nsp12 RNA-dependent RNA polymerase that was not present in pre-treatment samples and caused a 6-fold increase in resistance.
Although the history of molnupiravir and its recent use in the treatment of FIP has been described [6], there are currently no studies documenting natural or acquired resistance to molnupiravir. Molnupiravir has been shown to function as an RNA mutagen causing several defects in the viral genome [7]while remdesivir / GS-441524 is a non-binding RNA chain terminator [8], which suggests that its resistance profile will be different.
Overcoming resistance to GS-441524
Drug resistance can only be overcome in two ways: 1) by gradually increasing the dose of the antiviral to achieve drug levels in body fluids that exceed the resistance level, or 2) by using another antiviral that has a different mechanism of resistance, either alone or in combination. So far, the first option has been chosen, which has proved effective in many cases. However, resistance to GS-441524 may be complete or so high that increasing the dose is no longer effective. In such cases, the second option is increasingly used. Currently available alternatives to GS-441524, although still from an unapproved market, are GC376 and molnupiravir.
Antiviral drug treatment regimens for resistance to GS-441524
GC376 / GS-441524
The combined GS / GC regimen has been shown to be effective in cats treated with GS-441524 at doses up to 40 mg / kg without cure due to resistance to GS-441524. It is better to intervene as soon as resistance to GS-441524 is detected, which will allow the cat to be cured sooner and at lesser cost to the owner.
Rainman is the current supplier of GC376, which comes in 4 ml vials at a concentration of 53 mg / ml.
GS / GC dosage: The dose of GS (SC or PO equivalent) in combination antiviral therapy is the same as the dose needed to adequately control the symptoms of the disease. This is usually the last dose used before the end of treatment and relapse. To this dose of GS-441524, GC376 is added at a dose of 20 mg / kg SC q24h regardless of the form of FIP. This is sufficient for most cats, including many cats with neuro FIP, but some will need higher doses. If remission of clinical signs is not achieved or blood tests are of concern, the dose of GC376 is increased by 10 mg / kg up to 50 mg / kg SC q24h.
Duration of treatment: An eight-week combination GC / GS treatment is recommended, which is added to previous GS monotherapy. Some cats were cured at 6 weeks of combination therapy, but relapse is more likely than at 8 weeks.
Side effects: Most cats have no serious side effects. However, about one in five cats may experience nausea or discomfort at the beginning of treatment and sometimes longer. These side effects do not appear to be dose dependent and can be treated with anti-nausea drugs such as Cerenia, Ondansetron or Famotidine. Ondansetron appears to have performed better in some cats.
Molnupiravir
Molnupiravir has been reported to be effective in monotherapy in cats with FIP by at least one Chinese retailer GS-441524 [9], but there are no reports of its use in cats with resistance to GS-441524. However, resistance to GS-441524 is unlikely to spread to molnupiravir. The fact that it has been found to be effective as an oral medicine also makes it attractive for treatment alone, as many cats resistant to GS-441524 have suffered from injections for a very long time.
A field study of molnupiravir reportedly consisted of 286 cats with various forms of naturally occurring FIP, which were examined in pet clinics in the United States, the United Kingdom, Italy, Germany, France, Japan, Romania, Turkey and China. Among the 286 cats that participated in the trial, no deaths occurred, including seven cats with ocular (n = 2) and neurological (n = 5) FIP. Twenty-eight of these cats were cured after 4-6 weeks of treatment and 258 after 8 weeks. All treated cats remained healthy 3-5 months later, a period during which cats that were not successfully cured would be expected to relapse. These data provide convincing evidence of the safety and efficacy of molnupiravir in cats with various forms of FIP. However, we hope that this field study will be written in the form of a manuscript, submitted for review and published. Nevertheless, it is now sold to cat owners with FIP. At least one other major retailer of GS-441524 is also interested in using molnupiravir for FIP, indicating a demand for further treatment of cats with FIP antivirals.
Molnupiravir dosage: The safe and effective dosing of molnupiravir in cats with FIP has not been established based on closely controlled and monitored field studies such as those performed for GC376 [1] and GS-441524. [2]. However, at least one seller from China in his flyer for a product called Hero-2801 [9] provided some pharmacokinetic and field trial data for Molnuparivir in cats with naturally occurring FIP. This information does not clearly state the amount of molnuparivir in one of their “50 mg tablets” and the actual dosing interval (q12h or q24h?). The dose used in this study also seemed too high. Fortunately, an estimated starting dose of molnuparivir in cats with FIP can be obtained from the published studies of EIDD-1931 and EIDD-2801 [15] in vitro on cell cultures and laboratory and field studies GS-441524 [14,18]. Molnupiravir (EIDD-2801) has an EC50 of 0.4 μM / μl against FIPV in cell culture, while the EC50 of GS-441524 is approximately 1.0 μM / μl. [18]. Both have a similar oral absorption of approximately 40-50 %, so an effective subcutaneous (SC) dose of molnupiravir would be approximately half the recommended starting dose of 4 mg / kg SC q24h for GS441524. [14] or 2 mg / kg SC q24h. The oral (PO) dose would be doubled to account for less effective oral absorption per 4 mg / kg PO q24h dose. The estimated initial effective oral dose of molnupiravir in cats with FIP can also be calculated from the available Covid-19 treatment data. Patients treated with Covid-19 are given 200 mg of molnupiravir PO q12h for 5 days. This dose was, of course, calculated from a pharmacokinetic study performed in humans, and if the average person weighs 60-80 kg (70 kg), the effective inhibitory dose is 3,03.0 mg / kg PO q12h. The cat has a basal metabolic rate 1.5-fold higher than humans, and assuming the same oral absorption in both humans and cats, the minimum dose for cats according to this calculation would be 4.5 mg / kg PO q12h in neocular and non-neurological forms of FIP. If molnupiravir crosses the blood-brain and blood-brain barriers with the same efficacy as GS-441524 [3,18], the dose should be increased to 1,51.5 and 2,02.0-fold to ensure adequate penetration into aqueous humor and cerebrospinal fluid for ocular cats (88 mg / kg PO, q12 h), respectively. neurological FIP (~ 10 mg / kg PO, q12 h). These doses are comparable to those used in ferrets, where 7 mg / kg q12h maintains sterilizing blood levels of the influenza virus drug (1.86 μM) for 24 hours. [10]. Doses in ferrets of 128 mg / kg PO q12h caused almost toxic blood levels, while a dose of 20 mg / kg PO q12h caused only slightly higher blood levels. [10].
Molnupiravir / GC376 or Molnupiravir / GS-441524
Combinations of molnupiravir with GC376 or GS-441524 will be used more and more frequently, not only to synergy or complement their individual antiviral effects, but also as a way to prevent drug resistance. Medicinal cocktails have been very effective in preventing drug resistance in HIV / AIDS patients [11]. However, there is currently insufficient evidence on the safety and efficacy of the combination of molnupiravir with GC376 or GS-441524 as initial treatment for FIP.
Case studies
Rocky - DSH MN Neuro FIP
A 9-month-old neutered domestic shorthair cat obtained as a rescue kitten had several weeks of seizures with increasing frequency, ataxia and progressive paresis. The blood tests were unremarkable. FIP treatment was started at a dose of 15 mg / kg BID GS-441524, which decreased to SID for about a week. The cat showed improvement, seizures stopped, and mobility increased within 24 hours of starting treatment. Within 5 days of treatment, the cat was able to move again. However, approximately 2 weeks after the start of treatment, the cat experienced loss of vision, decreased mobility, recovery of seizures and difficulty swallowing. Dose adjustments of levetiracetam and prednisolone were made, as well as a change in the composition of GS-441524, followed by a temporary improvement in motility and swallowing and a reduction in seizures, but overall the cat's condition worsened. The dose of GS-441524 was gradually increased to 25 mg / kg, with little or no improvement. At this point, GS was taken orally at a dose of 25 mg / kg (estimated to be approximately 12.5 mg / kg) and within 3 days, the cat began to move, improved vision, and stopped seizures with increased energy and appetite. Improvement in cats continued for approximately 4 weeks with oral administration of GS-441524, then stopped for approximately 3 weeks before rapidly progressing paresis. Oral doses up to 30 mg / kg SC equivalent have been tested but have no effect. GS-441524 was then injected at a dose of 20 mg / kg and the cat was able to move again within 4 days with good appetite and energy. After 2 weeks, a dose of GC376 20 mg / kg BID was added to the dosing regimen. The cat terminated 6 weeks of the GS441524 and GC376 combination therapy and then discontinued the treatment. Although the cat has certain permanent neurological deficits, its condition is stable, it has good mobility, appetite and activity for 9 months after the end of antiviral treatment.
A four-month-old neutered domestic shorthair cat obtained as a rescue kitten was presented with a monthly history of lethargy and a progressive history of ataxia, hind limb paresis, spades, uveitis, anisocoria, and urinary and stool incontinence. Blood tests were mostly uncommon, with the exception of mild hyperglobulinemia. The A / G ratio was 0.6. The cat was treated with 10 mg / kg GS-441524 SC SID for 3 weeks. Activity, mentation and uveitis improved within 72 hours of starting treatment. During the first 2 weeks, a slow improvement in mobility and eye symptoms was observed, but then a plateau was reached. After 3 weeks, the dose of GS-441524 was increased to 15 mg / kg GS-441524 SC SID due to persistent neurological and ocular deficits. In addition, enlargement of the left eye due to glaucoma was noted at this time and the eye continued to swell until it was removed at week 8 of treatment. Due to persistent weakness / lack of pelvic coordination and increasing lethargy, dose GS-441524 was increased to 20 mg / kg SC SID [or equivalent oral dose] at week 9 and 20 mg / kg SC BID was added to the regimen a few days later. GC376. Significantly increased activity and willingness to jump on elevated surfaces occurred within 48 hours of starting GS376 treatment. The combination treatment of GS-441524 and GC376 was maintained for 8 weeks. The cat has residual incontinence problems after treatment, but is otherwise clinically normal 6 months after treatment.
Boris - Maine Coon MI wet eye FIP
The five-month-old intact (uncastrated) Maine Coon cat, obtained from the breeder, had lethargy, anorexia, abdominal ascites, cough, anemia and neutrophilia. No biochemical analysis was performed to establish the diagnosis. The cat was treated with 6 mg / kg GS-441524 SC SID for 8 weeks. After six weeks of treatment, X-rays revealed nodules in the lungs, and after 8 weeks, hyperglobulinemia persisted. The GS-441524 dose was then increased to 8 mg / kg SC SID for 4 weeks. There was little improvement in blood tests and X-rays and the dose of GS-441524 was increased to 12 mg / kg SC SID over 4 weeks, followed by an increase to 17 mg / kg over 11 weeks, 25 mg / kg over 4 weeks and 30 mg / kg for 4 weeks. After 25 weeks of treatment, ultrasound revealed pleural abnormalities on the left side and X-rays showed no improvement in the pulmonary nodules. In addition, uveitis and retinal detachment have been reported in the right eye. Pulmonary aspirates that showed FIP-compliant inflammation were collected. After 33 weeks of treatment, 20 mg / kg SC BID GC376 was added to the regimen and the combined treatment of GS-441524 and GC376 was continued for 12 weeks. Increased activity was noted over several days. Over the course of 5 weeks, the weight gain accelerated, the cough subsided and the energy level increased. Blood tests showed an improvement in the A / G ratio, and chest X-rays showed a reduction in the lungs. After 84 days of combination antiviral therapy, the A / G ratio was 0.85 and the cat appeared clinically normal. The cat is currently 3 months after treatment.
References
Pedersen NC, Kim Y, Liu H, Galasiti Kankanamalage AC, Eckstrand C, Groutas WC, Bannasch M, Meadows JM, Chang KO. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J Feline Med Surg. 2018; 20 (4): 378-392.
Pedersen NC, Perron M, Bannasch M, Montgomery E, Murakami E, Liepnieks M, Liu H. efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. J Feline Med Surg. 2019; 21 (4): 271-281.
Perera KD, Rathnayake AD, Liu H, et al. Characterization of amino acid substitutions in feline coronavirus 3C-like protease from a cat with feline infectious peritonitis treated with a protease inhibitor. J. Vet Microbiol. 2019; 237: 108398. doi: 10.1016 / j.vetmic.2019.108398
Agostini ML, Andres EL, Sims AC, et al. Coronavirus susceptibility to the antiviral remdesivir (GS5734) is mediated by the viral polymerase and the proofreading exoribonuclease. MBio 2018; 9. DOI: 10.1128 / mBio.00221-18.
Pedersen NC. 2021. The neurological form of FIP and GS-441524 treatment. https://sockfip.org/the-neurological-form-of-fip-and-gs-441524-treatment/
Pedersen NC. The long history of beta-d-n4-hyroxycytidine and its modern application to treatment of covid019 in people and FIP in cats. https://sockfip.org/the-long-history-of-beta-d-n4-hydroxycytidineand-its-modern-application-to-treatment-of-covid-19-in-people-and-fip-in- cats /.
Agostini, ML et al. Small-molecule antiviral beta-dN (4) -hydroxycytidine inhibits a proofreading-intact coronavirus with a high genetic barrier to resistance. J. Virol. 2019; 93, e01348.
Warren, TK et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016; 531, 381–385.
FIP Warriors CZ / SK - EIDD-2801 (Molnupiravir) https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/
Toots M, Yoon JJ, Cox RM, Hart M, Sticher ZM, Makhsous N, Plesker R, Barrena AH, Reddy PG, Mitchell DG, Shean RC, Bluemling GR, Kolykhalov AA, Greninger AL, Natchus MG, Painter GR, Plemper RK . Characterization of orally efficacious influenza drug with high resistance barrier in ferrets and human airway epithelia. Sci Transl Med. 2019; 11 (515): eaax5866.
Zdanowicz MM. The pharmacology of HIV drug resistance. Am J Pharm Educ. 2006; 70 (5): 100.doi: 10.5688 / aj7005100
Gandhi, S, Klein J, Robertson A, et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. medRxiv, 2021.11.08.21266069AID