Department of Microbiology and Immunology E-mail: ha363@cornell.edu Sponsor: Cornell Feline Health Center Research Grants Program Title: Two Vaccine Platforms to Prevent Feline Coronavirus Disease Project Amount: $69,920 Project Period: July 2021 to June 2022
DESCRIPTION (provided by applicant):
While most cats infected with Feline Coronavirus (FCoV) develop mild to inapparent diarrheal disease, a subset of them develop the devastating and deadly feline infectious peritonitis (FIP). FCoV can spread via fecal-oral or respiratory routes, particularly in cat shelter environments. Coronaviruses have three envelope glycoproteins, S, E, and M, but the surface protein (S) is in charge of viral entry. S binds the cell surface receptor and then merges the viral membrane to the cell plasma or endosomal membranes, causing viral entry. S also causes cell-cell fusion (syncytia) post-infection. The S protein of most coronaviruses is also highly immunogenic. The devastating FIP disease begs the development of protective vaccines. We identified a small molecule, XM-01, that embeds within viral membranes and inhibits membrane fusion. Importantly, this novel method of inhibition renders virions noninfectious, while maintaining the native conformations of the surface glycoproteins, ideal for eliciting effective immune responses against such viral glycoproteins. Remarkably, vaccination with XM-01-treated influenza virions yielded an increase in neutralizing antibodies and survival rate, and a decrease in morbidity and mortality upon viral challenge in a mouse model, as compared to the traditional formalin-inactivated influenza vaccine. Thus, our Aim 1 will be to determine whether XM-01 can be used to develop a FeCoV inactivated vaccine. Importantly our recent preliminary data includes already determined conditions for complete FCoV inactivation. We will optimize XM-01 inactivation of FCoV in preparation to determine whether this vaccine can yield a robust immune response against this virus. Additionally, our lab has successfully used replication-incompetent vesicular stomatitis virus (VSV)-based pseudotyped virions to vaccinate and protect hamsters against Nipah, Hendra, and Ebola virus diseases with 100% safety and 100% efficacy (manuscript in final revision for Nature Publishing Journals Vaccines). Our Aim 2 will use the replication-incompetent VSV system to develop a vaccine against FCoV. We will optimize incorporation of FCoV-S into VSV virions in preparation to determine whether this vaccine can yield a robust immune response against this virus. As both inactivated and replication-incompetent virions vaccine platforms have been successfully used to prevent other viral diseases, the completion of our Aims will allow our vaccine platforms to readily advance to vaccination clinical trials/licensing.
Infectious feline peritonitis (FIP) is a fatal disease caused by feline coronavirus (FCoV) infection. FCoV can be divided into serotypes I and II. The virus that causes FIP (FIPV) is said to occur sporadically and does not often spread from one cat to another. An outbreak in one animal shelter in Taiwan was recently confirmed. FCoV from all cats in this shelter was analyzed to determine the epidemiology of this outbreak. Thirteen of the 46 (28,2%) cats with typical FIP symptoms were identified. Of these, FIP was confirmed in seven cats by necropsy or histopathological examination. Despite the fact that in this environment with more cats, more than one FCoV was identified, eight cats with symptoms of FIP were reliably found to be infected with FCoV type II. Sequence analysis revealed that FIPV type II, found from feline faeces, body effusions and granulomatous tissue homogenate from cats that underwent FIP, contained identical recombination in all cases. WITH gene. Two cats that succumbed to FIP were found to have an identical nonsense mutation in 3c gene. The excretion of this type II virus in faeces of the effusive form of FIP can be detected up to six days before the animal dies. In general, our data demonstrate that horizontal transmission of FIPV is possible and that FIP cats may pose a potential risk to other cats living in the same environment.
Introduction
Infectious feline peritonitis (FIP) is a fatal disease of cats caused by feline coronavirus (FCoV) infection. FCoV is an enveloped RNA virus that belongs to the species Alphacoronavirus, family Coronaviridae and in order Nidovirales. The size of the FCoV genome is approximately 28.9 kb, including the nonstructural replication gene; four structural genes that encode spike (S), envelope, membrane, and nucleocapsid proteins; and five helper / nonstructural genes 3abca 7ab[1].
Feline coronaviruses cause mild, invisible, and transient bowel infections and are ubiquitous among cat populations worldwide [2]. They occur in two serotypes, I and II [man]3]. Type I FCoV predominates here, while type II virus represents only 2-30% infections [4–8]. Following the accumulation of genetic evidence, it is apparent that FCoV type II was formed by two homologous recombinations between FCoV type I and canine coronavirus CoV (CCoV) [9,10]. Both serotypes can mutate in the host, lead to macrophage tropism and a systemic disease called infectious feline peritonitis [cat]2,11,12]. Due to poor virus shedding in FIP studies in cats, mutant FIP viruses (FIP-inducing FCoV, FIPV) appear to be contained only in diseased tissues and are not naturally transmitted in cat-to-cat contact [2,11,13,14].
In this article, we report an epizootic FIP in a shelter in Taiwan that was caused by a new Type II FCoV. Epidemiological and molecular examination of isolates from various healthy and sick cats from this shelter strongly suggests that the virus was introduced by moving kittens from another shelter with subsequent horizontal spread to adult cats with which the new kittens shared the shelter.
Materials and methods
Animals and sampling
A total of 46 cats from a private shelter were included in this study, which ran from September 2011 to August 2012. This shelter houses adult cats and from time to time a few kittens. All the cats were either strayed or rescued, and some of them were obtained from the homes of various private rescue stations where the rescued cats were temporarily housed. Before the onset of the disease, all cats lived together in an indoor environment without cages, sharing food, drink and toilets. Some cats were siblings, others were not related to them (Table 1).
Table 1 Information on all cats from this shelter in which FIP was suspected and in which the disease was confirmed
Ascites, jaundice, granulomatous lesions in the kidney, fibrinous peritonitis
Effusive
8
6m
July 11, 2011
ON THE
December 14, 2011
Granulomatous changes in the kidneys, liver, lungs, brain and eyes
Non-fusible
9
2y
Resident
ON THE
December 28, 2011
Ascites, pleural effusion and pericardial effusion, granulomatous changes in the kidneys, liver and intestine.
Effusive / non - fusive
10 b
3m
July 11, 2011
ON THE
November 5, 2011
Granulomatous changes in the kidneys, liver and omentum
Non-fusible
11 c
1y6m
Resident
ON THE
February 14, 2012
Ascites and pleural effusion, jaundice, fibrinous peritonitis, granulomatous changes in the kidneys, liver, lungs and spleen.
Effusive / non - fusive
12 c
1y6m
Resident
ON THE
March 19, 2012
Jaundice, fibrinous peritonitis, granulomatous changes in the thoracic and abdominal walls, kidneys, liver, lungs, spleen omenta and eyes.
Effusive / non - fusive
13
1y7m
Resident
ON THE
April 13, 2012
Jaundice, enlargement of the liver and mesenteric lymph nodes, granulomatous changes in the kidneys and lungs.
Non-fusible
1 Age of cats at the time of clinical signs of FIP. 2 Not available. a, b, c : siblings.
Faeces or rectal samples were taken from all asymptomatic cats at least once to monitor for FCoV. Body swabs, blood samples, swab specimens, including rectal, nasal, oral and conjunctival specimens, were taken as standard from cats that already showed signs of the disease or were suspected of having FIP. In addition to supportive care, cats with suspected FIP were treated with prednisolone (Prelon®, YF Chemical Corp., New Taipei City, Taiwan), benazepril (Cibacen®, Novartis, Barbera del Valles, Spain) and recombinant human interferon alpha (Roferon®-A). , Roche, Basel, Switzerland). Cats that succumbed to the disease were necropsied for pathological confirmation. During necropsy, body exudates were first removed with a needle and syringe, followed by swabs, blood, urine and granulomatous lesions on the internal organs. All samples were frozen at -20 ° C until use. All samples were tested for FCoV nested reverse transcription polymerase chain reaction (RT-nPCR) [man]15]. Samples with positive results were subsequently subjected to further analysis.
Sample preparation and reverse transcription
Swab samples were suspended in 1 ml of water treated with 0.1% diethyl pyrocarbonate (DEPC). Stool samples were suspended with 9x treated water 0.1% DEPC by vortexing. The suspension was centrifuged and the supernatant was transferred to a new tube. About 0.5 g of tissue was frozen and then crushed with a mortar and pestle in the presence of 2 ml of Trizol [16]. Total RNA was extracted from 300 μl of swab suspension, whole blood, faeces suspension, tissue homogenate and body effusion using Trizol. Twenty-one microliters of isolated RNA was reverse transcribed with specific primer N1 (5′-gctacaattgtatcctcaac-3 ′) or P211 [15] with Moloney mouse leukemia reverse transcription (Invitrogen, CA, USA). The reaction was incubated at 37 ° C for 60 min, at 72 ° C for 15 min and finally at 94 ° C for 5 min.
FCoV type determination by nested PCR
Nested PCR was performed for FCoV typing according to the procedures of Addie et al. [5] with a slight modification. After reverse transcription, 5 μl of complementary DNA was added to 25 μl of PCR mix (Invitrogen, CA, USA) according to the manufacturer's instructions for the following primer sets: S1 and Iffs to determine FCoV type I and S1 and Icfs to determine FCoV type II. Nested PCR was performed on 2 μl of the first PCR product using nested primers. The expected size of the second PCR achieved for type I and type II FCoV was 360 and 218 bp. RT-nPCR products were electrophoresed and then the target DNA fragments were purified (Geneaid Biotech, Ltd, Taipei) and sequenced (Mission Biotech, Taipei, Taiwan) - from both orientations.
Gene amplification, sequencing and analysis 3a and 3c from FCoV type II
For amplification 3a of the FCoV type II gene from FIP cats, a set of specific primers was designed that is able to amplify from WITH type II gene to gen 3a. Complementary DNA, amplified with a primer set, targeted the 3 'end WITH FCoV type II gene (Icfs) and 5 ′ end 3a FCoVe gene (3aR2: 5′-caccaaaacctatacacacaag-3 ′). The temperature cycle was as follows: 5 minutes preheating at 94 ° C; 35 cycles of denaturation at 94 ° C for 20 s, annealing at 50 ° C for 20 s and extension at 72 ° C for 30 s; and final extension at 72 ° C for 5 minutes. This was followed by a second series of amplification using primers nIcfs and 3aR2; the expected product size was about 600 bp. Amplicons were electrophoresed, purified, and sequenced from both orientations to confirm nucleotide sequences.
For amplification 3c of the FCoV type II gene from FIP cats, a set of specific primers was designed that is able to amplify from WITH type II gene to gen 3c. Complementary DNA was amplified with forward primer (Icfs) and reverse primer (E68R: 5′-aatatcaatataattatctgctgga-3 ′ and N21R: 5′-gttcatctccccagttgacg-3 ′, respectively). The temperature cycle was as follows: 5 minutes preheating at 94 ° C; 40 cycles of denaturation at 94 ° C for 30 s, annealing at 46 ° C for 30 s and extension at 72 ° C for 90 s; and final extension at 72 ° C for 7 minutes. Following a second series of amplification using primers nIcfs and E68R, the products were electrophoresed, purified and sequenced from both orientations to confirm nucleotide sequences.
Phylogenetic analysis and recombinant analysis of FCoV type II
Several sequence alignments were performed using ClustalW 2.0 with manual editing in EditSeq (DNASTAR, Madison, USA). Phylogenetic analyzes were performed using MegAlign, version 7.2.1 (DNASTAR, Madison, USA). Bootscan and similar graphs were compiled using SimPlot 3.5.1 software (SCRoftware, Baltimore, USA).
The results
Confirmation of the FIP outbreak in the cat shelter
The shelter has been operating for three and a half years. Prior to August 2011, there were no records of FIP. The kittens (cats 1, 3, 4, 8 and 10) were moved to this shelter between June and July 2011. After arrival, these kittens played together and lived together with adult cats that lived here before. Prior to the outbreak, the kittens were individually taken to a veterinarian for vaccination and adoption visits. Fever was first detected in four kittens (cats 1, 3, 4, 5) within a few days (from 15 to 18 August) (Table 1). Clinical symptoms, e.g. fever, anorexia, neurological symptoms, shortness of breath and enlargement of the abdomen were observed over the next two months and the kittens gradually died between 1 September and 22 October (Table 1). Shelters from the shelter asked for our help on September 27. All cats housed in the shelter for a long time were immediately examined for FCoV using the RT-nPCR method. All FCoV-positive cats were isolated and kept separately. Nevertheless, starting in September, adult cats with FIP (cats 7-13) showed clinical signs similar to kittens, and all of these cats later died.
Six kittens (cats 1-6) with body effusions or neurological symptoms that succumbed in the first two months were not confirmed for necropsy (Table 1). Cat 1 was once brought to our teaching hospital and ascites (free fluid in the abdominal cavity) was taken from her. In cats 7-13, typical symptoms were found, namely ascites or pleural effusions in the body cavity (effusive FIP) and granulomatous lesions in some organs, especially in the kidneys, nuclei, lungs, omentum (forecourt) and eyes (non-effusive FIP). In cats 9, 11 and 12, necropsy showed a mixed form of the disease (Table 2) 1).
A total of 13 of the 46 cats (28.3%) died between September 2011 and April 2012 at FIP. At this time, 33 cats (71.7%) appeared to be clinically healthy and 26 of these asymptomatic cats (78.7%) were positive at least once for FCoV - detected from faeces using the RT-nPCR method. The other seven of these asymptomatic cats were negative for FCoV (Table 2) 2).
Table 2 Detection of the occurrence and type of FCoV from faeces samples in healthy cats from the same shelter
Hot girl
FCoV
Type
Oct. 2011
Feb. 2012
Jun. 2012
Jul. 2012
14
++
++
++
+
untypable
15
–
+
–
untypable
16
++
–
–
untypable
17
++
++
+
++
I
18
++
++
++
++
I
19
–
–
+
untypable
20
–
–
+
untypable
21
–
–
–
22
++
++
–
untypable
23
+
++
–
+
I
24
–
+
–
untypable
25
++
++
+
+
I
26
–
+
–
untypable
27
++
++
+
+
I
28
++
++
++
+
I
29
–
–
–
30
–
++
++
–
I
31
–
–
32
+
++
–
–
I
33
–
++
–
untypable
34
++
I
35
–
+
+
untypable
36
++
++
+
–
I
37
–
38
+
untypable
39
++
+
+
I
40
–
+
–
untypable
41
+
–
+
untypable
42
+
–
untypable
43
–
44
–
45
–
46
+
untypable
++: FCoV detected in the first round of PCR. +: FCoV detected only in nested PCR.
FIPV type II was found in all cats that succumbed to FIP
In order to further investigate the relationship between these seven histopathologically confirmed FIP cats, the amplified DNA was typed, sequenced and analyzed. FIPV type II was detected in all eight animals that succumbed to FIP, from swabs, faeces, urine, body effusions, cerebrospinal fluid, and tissue homogenates (Table 3). Type II viruses that cause FIP have been found not only in diseased tissue but also in faeces samples (cats 7, 11, 12 and 13), nasal / oral / conjunctival swab samples (cats 7, 8, 9, 11 and 12). ) and in urine collected by cystocentesis (cat 11) (Table 3). Although no necropsy was performed, ascites from cat 1 - the first cat to die in the shelter at FIP - were available for analysis. This cat was confirmed to be infected with type II virus. In healthy animals, only type I or FCoV was detected from faeces samples without type determination (Table 2) 2). Cats 8, 9 and 13 were infected with both types of FCoV (Table 2) 3). Although it has been found that in this environment with many cats there is more than one type of FCoV, ie. type I, II or non-typed viruses, FCoV type II infection was found in all eight FIP cats, whereas this was not the case in healthy animals (Tables 2 and33).
Table 3 Characteristics 3c FCoV genes obtained from different samples of FIP cats
Hot girl
FCoV genotype
WITH instead of gene crossing
Integrity 3c geneb
NIGHT
R / F
U
A / P
CSF
Li
Lu
Ki
Br
Sp
Int
R / F
A / P
Li
Lu
Ki
Br
Sp
1
II
4250and
intact
7
II
II
II
II
II
II
II
II
4250
intact
intact
intact
intact
intact
8
II
I
+
II
II
+
–
–
9
II
I
II
+
II
II
II
+
4250
G210 *
G210 *
G210 *
10
+
+
II
II
II
4250
intact
11
II
II
II
II
+
II
II
II
+
4250
E47 *
12
II
II
II
II
+
II
II
II
+
4250
G210 *
G210 *
13
I / II
+
+
+
II
II
+
4250
Q218 *
NIGHT, nose / mouth / conjunctival swabs; R / F, rectal swabs or stool samples; A / P, ascites or pleural effusion; CSF, cerebrospinal fluid; Li, liver; Lu, lungs; Ki, kidney; Br, brain; Sp, spleen; Int, gut. +: FCoV positive, but virus type cannot be determined. -: FCoV negative. a: FCoV / NTU2 / R / 2003; GenBank: DQ160294. b: E47 *, G210 * and Q218 *: truncated 3c proteins with premature stop codons at amino acids 47, 210 and 218 were found.
FIPV type II of the same origin was found in cats that succumbed to FIP
Recombination at the 3 ′ end WITH of the putative recombination site at nucleotide 4250 was determined in all FCoV type II animals obtained from body effusions and tissue homogenates in cats 1, 7, 9, 10, 11, 12 and 13 (Additional set 1) (Table 3). Sequences above this site show greater similarity to CCoV, whereas sequences beyond this site were more similar to type I FCoV (Fig. 1). 1). Indeed, these findings suggest that FCoV type II, found in all FIP cats, has a common origin.
Figure 1 FIPV recombination from cats 1, 7, 9, 10, 11, 12 and 13 on the S gene. Alignment of the 3 ′ end of the S gene with subsequent FCoV genes isolated from seven FIP cats with FCoV type I and CCoV. The light and dark shaded regions include greater similarity to CCoV and FCoV type I. The predicted recombination event occurred at nucleotide 4250 based on comparison to FCoV NTU2 and is indicated by an arrow. Sequences were obtained from FIPV found in individual samples and tissues and are summarized. NIGHT: swabs from the nose / mouth / conjunctiva; RS: rectal swabs; As: ascites; PE: pleural effusion; Li: liver; Lu: lungs; Ki: kidneys; Br: brain; Sp: spleen; dbd: days before death. GenBank accession number: FCoV C1Je (GenBank: DQ848678), FCoV Black (GenBank: EU186072), FCoV NTU2 (GenBank: DQ160294) and CCoV NTU336 (GenBank: GQ477367).
Identical nonsensical mutation on 3c The gene was found in two cats that succumbed to FIP
In order to further analyze the relationship of these FIPVs, they were 3c genes, a proposed virulence-associated FIP, are amplified from the disease-causing FCoV type II. Mutated 3c genes with identical premature stop codon at nucleotides 628-630 (amino acids 210, G210 *) were found in two FIP cats, cat 9 (ascites, spleen and brain) and 12 (ascites and rectal swabs from the day the cat died and four days previously) (Fig. 2A). It is worth noting that FIPV, obtained from cat 12, showed the same nonsense mutation as the virus in its ascites. Intact 3c the genes were discovered in cats 1, 7 and 10, which had previously succumbed to FIP. Two other clear / different nonsense mutations were found in cats 11 (E47 *) and 13 (Q218 *) (Fig. 1). 2AB, Table 3).
Figure 2: Alignment of complete FIPV 3c genes from cats 1, 7, 9, 10, 11, 12 and 13. (A) The full length 3c genes analyzed in this study were aligned with FCoV type I, FCoV NTU2. The sequences were obtained from FIPV found in individual samples and tissues and are listed together. The box represents the identified premature stop codons. (B) The diagram shows the location of premature stop codons (PT) of gene 3c from different samples from different FIP cats.
FIPV type II excretion can be detected in the terminal phase in FIP cats
The occurrence of FCoV was continuously analyzed to elucidate a possible route of FIPV secretion and transmission. Disease-associated FCoV type II was found to be excreted by the nasal / oral / conjunctival route and faeces (Table 4). Faecal and nasal / oral / conjunctival type II shedding can be detected from day 6 (cat 11) and from day 4 (cat 12) before death. Viremia can be detected during the terminal stage in cats suffering from FIP up to 18 days before death, and concomitant faecal excretion was detected in one cat (cat 12) (Table 4).
Table 4 Excretion and serotypes of feline coronavirus detected in FIP cats in a cat shelter
Hot girl
Sample
Days before death
−80
−66
−60
−57
−50
−43
−36
−29
−25
−23
−20
−18
−14
−12
−8
−6
−4
0*
9
Feces
I
I
II
NIGHT tampons
II
Viremie
II
+
Efuze
II
II
II
11
Feces
–
–
–
II
II
NIGHT tampons
–
–
II
Viremie
–
–
–
–
–
Efuze
+
II
12
Feces
–
+
–
–
–
–
–
–
–
–
–
–
+
II
II
NIGHT tampons
–
–
–
–
–
–
–
–
–
–
II
II
Viremie
–
–
–
–
–
–
–
–
–
II
+
+
–
Efuze
II
II
+: FCoV positive; -: FCoV negative. I, II: FCoV type I or type II. *: Samples were taken immediately before euthanasia, except for cat 12, which were sampled after death.
Discussion
The possibility of horizontal transmission is generally questioned in FIP because (i) the occurrence of FIP is sporadic and it is common for only one of them to develop FIP in an environment with a large number of cats [2]; (ii) internal mutation theory, which describes that FIPV is a mutant generated from enteric FCoV in one cat [12,17]; (iii) there is insufficient evidence that the mutant FIPV is eliminated from FIP cats; and (iv) mutations 3c gene is unique for every FIP cat [man]11,13,18]. The current belief is that cats that have succumbed to FIP do not excrete and pass FIPV to other cats [11,13,14,18–20]. Our data indicate that this outbreak of FIP was caused by viruses of the same origin. First, all cats that died of FIP had a type II infection, and recombination of these seven type II viruses was located at the same site. Recombination of type II viruses currently available in the genetic bank, i.e. FIPV 79-1146, FCoV 79-1683 and FCoV NTU156, were all unique, specific and occurred independently [9,10]. Second, FIPV, found in three kittens that died within the first two months after the onset of fever, had an intact 3c gene, whereas viruses from cats that survived longer (died four to eight months later) all contained a nonsensical mutation, i. G210 * (cats 9 and 12), E47 * (cat 11) and Q218 * (cat 13). Because the three nonsense mutations found in FIPV in these animals were all located at different sites, the viruses that originally infected these cats should be intact. 3c gene - similar to the virus found in kittens that died earlier. Following infection, local mutations occurred during virus replication in individual cats, resulting in FIPV with 3c a gene that carries meaningless mutations in different places. The finding that viruses, which were identified not only in tissues but also in faecal samples in two cats (cats 9 and 12), had an identical mutation in 3c gene, further confirmed that there was a horizontal transfer (Table 2) 3). Taken together, all of these findings demonstrated that highly virulent FIPV spread horizontally from one animal to another.
This is the first report of an FIPV type II outbreak with evidence of horizontal disease-causing FCoV transmission. The FIP broke out after five kittens (cats 1, 3, 4, 8 and 10) entered this shelter between June and July 2011. Because causative type II viruses with a specific genetic marker in the S gene have been confirmed as feline and canine coronavirus recombination, and some of the kittens that died earlier were found to have lived together or next to dogs between rescue and transport to the shelter. of these kittens may have been the source of this type II virus. Dogs and especially young dogs often shed large amounts of canine coronavirus in their faeces in shelters, and recombination between feline-canine and canine-feline coronavirus is already well documented [man]21–23]. In addition, type II causative viruses have been detected in a number of excreta and secretions in cats that have died of FIP (Table 3), demonstrating that it is possible to spread between cats.
Although immediately after the first examination of all animals from this FCoV shelter, FCoV-secreting cats were housed in separate cages and transmission subsequently ceased, mortality at the onset of the disease was high (28%, 13/46). The results of three studies that looked at the outbreak of FIP have been reported earlier. The results of a four-year study conducted at a nearby cat kennel showed an average mortality of 17.3% [24]; the mortality rate from a ten-year study conducted at a nearby kennel was 29.4% (5/17) [25]. Another epidemic study conducted in seven kennels / shelters revealed >10% mortality [20]. The high incidence of FIP in these closed breeding stations could be influenced by genetically predisposed breeding animals. In our study, only a few FIP cats in this shelter were siblings and the other cats were not genetically related. Our study shows that even without the influence of genetic predisposing factors, FIP mortality can be high in a confined environment with a large number of cats if the spread of FCoV, which causes the disease, remains undetected.
In this environment with a large number of cats, three FIP cats were infected not only with FCoV type II, but also co-infected with FCoV type I (Table 3). Type I FCoV was found only in faecal samples, while type II FCoV was found in various samples, including body effusions, granulomatous tissue homogenates, and cerebrospinal fluid. This finding indicates that FCoV type II was a major cause of FIP in these doubly infected animals. This finding is consistent with our previous finding that FCoV type II infection is significantly associated with FIP [4].
The presence of FCoV in whole blood in the terminal phase has been identified previously [26,27]; however, to our knowledge, the presence of FIPV in faeces prior to the final stage of the disease was not published anywhere until our study. The excretion of this type II virus in faeces and by the nasal / oral / conjunctival route can be detected in the effusive form of FIP up to six days before the death of the animal. Another experimental study of the infection showed that inoculated viruses could not be detected until about two weeks after inoculation, before clinical signs of the disease developed [14]. In summary, FIPV transmission could occur at the beginning, before the manifestations of the disease and in the terminal phase. When the disease broke out in our case, all the cats were initially placed together in an open room. After seven cats gradually succumbed to the disease, all FCoV-positive cats were housed separately in cages and kept separately. Isolation probably inhibited disease transmission. This outbreak of disease, which killed 13 cats, allowed us to make it clear that FIPV can be transmitted horizontally and to show that the isolation of sick cats should be taken into account in an environment where more cats are present.
Competitive interests
The authors claim that they have no competitive interests.
Contributions and contributions of authors
YTW performed sampling and preparation, FCoV detection, type determination, amplification 3c gene and other analyzes and compiled a manuscript. The BLS supervised the sampling and treatment of all FIP animals and contributed to the compilation of the manuscript. LEH participated in the amplification 3c gene, genetic analysis and manuscript preparation. The LLC devised the study, participated in the design of the study, coordinated and participated in the preparation of the manuscript. All authors read and approved the final version of the manuscript.
Additional material
Additional file 1:
FIPV recombination site analysis in cats 1, 7, 9, 10, 11, 12 and 13 at WITH gene. Analysis of the plot similarity using the Kimur (two-parameter) distance model, the model of adjacent interconnected trees, and 100 replicates of the bootstrap showed that recombination had occurred and the putative crossing point is indicated by an arrow.
Thanks
The authors would like to thank the caregivers in the mentioned cat shelter, without whose help this study would not have been possible.
Literature
Lai MMC, Perlman S, Anderson LJ. In: Fields virology. Knipe DM, Howley PM, Griffin DE, Lamb RA, Martin MA, Roizman B, Straus SE, editor. Philadelphia: Lippincott Wiilliams & Wikins; 2007. Coronaviridae; pp. 1305–1335.
Pedersen NC. A review of feline infectious peritonitis virus infection: 1963-2008. J Feline Med Surg. 2009; 44: 225–258. doi: 10.1016 / j.jfms.2008.09.008. [PubMed] [Cross Ref]
Pedersen NC, Black JW, Boyle JF, Evermann JF, McKeirnan AJ, Ott RL. Pathogenic differences between various feline coronavirus isolates. Adv Exp Med Biol. 1984; 44: 365-380. doi: 10.1007 / 978-1-4615-9373-7_36. [PubMed] [Cross Ref]
Lin CN, Su BL, Wang CH, Hsieh MW, Chueh TJ, Chueh LL. Genetic diversity and correlation with feline infectious peritonitis of feline coronavirus type I and II: a 5-year study in Taiwan. Vet Microbiol. 2009; 44: 233–239. doi: 10.1016 / j.vetmic.2008.11.010. [PubMed] [Cross Ref]
Addie DD, Schaap IA, Nicolson L, Jarrett O. Persistence and transmission of natural type I feline coronavirus infection. J Gen Virol. 2003; 44: 2735–2744. doi: 10.1099 / vir.0.19129-0. [PubMed] [Cross Ref]
Benetka V, Kubber-Heiss A, Kolodziejek J, Nowotny N, Hofmann-Parisot M, Mostl K. Prevalence of feline coronavirus types I and II in cats with histopathologically verified feline infectious peritonitis. Vet Microbiol. 2004; 44: 31–42. doi: 10.1016 / j.vetmic.2003.07.010. [PubMed] [Cross Ref]
Hohdatsu T, Okada S, Ishizuka Y, Yamada H, Koyama H. The prevalence of types I and II feline coronavirus infections in cats. J Vet Med Sci. 1992; 44: 557–562. doi: 10.1292 / jvms.54.557. [PubMed] [Cross Ref]
Kummrow M, Meli ML, Haessig M, Goenczi E, Poland A, Pedersen NC, Hofmann-Lehmann R, Lutz H. Feline coronavirus serotypes 1 and 2: seroprevalence and association with disease in Switzerland. Clin Diagn Lab Immunol. 2005; 44: 1209–1215. [PMC free article] [PubMed]
Lin CN, Chang RY, Su BL, Chueh LL. Full genome analysis of a novel type II feline coronavirus NTU156. Virus Genes. 2013; 44: 316–322. doi: 10.1007 / s11262-012-0864-0. [PubMed] [Cross Ref]
Herrewegh AA, Smeenk I, Horzinek MC, Rottier PJ, de Groot RJ. Feline coronavirus type II strains 79-1683 and 79-1146 originate from a double recombination between feline coronavirus type I and canine coronavirus. J Virol. 1998; 44: 4508–4514. [PMC free article] [PubMed]
Rottier PJ, Nakamura K, Schellen P, Volders H, Haijema BJ. Acquisition of macrophage tropism during the pathogenesis of feline infectious peritonitis is determined by mutations in the feline coronavirus spike protein. J Virol. 2005; 44: 14122–14130. doi: 10.1128 / JVI.79.22.14122-14130.2005. [PMC free article] [PubMed] [Cross Ref]
Chang HW, de Groot RJ, Egberink HF, Rottier PJ. Feline infectious peritonitis: insights into feline coronavirus pathobiogenesis and epidemiology based on genetic analysis of the viral 3c gene. J Gen Virol. 2010; 44: 415–420. doi: 10.1099 / vir.0.016485-0. [PubMed] [Cross Ref]
Stoddart ME, Gaskell RM, Harbor DA, Gaskell CJ. Virus shedding and immune responses in cats inoculated with cell culture-adapted feline infectious peritonitis virus. Vet Microbiol. 1988; 44: 145-158. doi: 10.1016 / 0378-1135 (88) 90039-9. [PubMed] [Cross Ref]
Herrewegh AA, de Groot RJ, Cepica A, Egberink HF, Horzinek MC, Rottier PJ. Detection of feline coronavirus RNA in feces, tissues, and body fluids of naturally infected cats by reverse transcriptase PCR. J Clin Microbiol. 1995; 44: 684–689. [PMC free article] [PubMed]
Chomczynski P, Sacchi N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem. 1987; 44: 156–159. [PubMed]
Poland AM, Vennema H, Foley JE, Pedersen NC. Two related strains of feline infectious peritonitis virus isolated from immunocompromised cats infected with a feline enteric coronavirus. J Clin Microbiol. 1996; 44: 3180–3184. [PMC free article] [PubMed]
Pedersen NC, Liu H, Scarlett J, Leutenegger CM, Golovko L, Kennedy H, Kamal FM. Feline infectious peritonitis: role of the feline coronavirus 3c gene in intestinal tropism and pathogenicity based upon isolates from resident and adopted shelter cats. Virus Res. 2012; 44: 17–28. doi: 10.1016 / j.virusres.2011.12.020. [PubMed] [Cross Ref]
Foley JE, Poland A, Carlson J, Pedersen NC. Patterns of feline coronavirus infection and fecal shedding from cats in multiple-cat environments. J Am Vet Med Assoc. 1997; 44: 1307–1312. [PubMed]
Foley JE, Poland A, Carlson J, Pedersen NC. Risk factors for feline infectious peritonitis among cats in multiple-cat environments with endemic feline enteric coronavirus. J Am Vet Med Assoc. 1997; 44: 1313–1318. [PubMed]
Stavisky J, Pinchbeck G, Gaskell RM, Dawson S, German AJ, Radford AD. Cross sectional and longitudinal surveys of canine enteric coronavirus infection in kennelled dogs: a molecular marker for biosecurity. Infect Genet Evol. 2012; 44: 1419–1426. doi: 10.1016 / j.meegid.2012.04.010. [PubMed] [Cross Ref]
Decaro N, Mari V, Elia G, Addie DD, Camero M, Lucente MS, Martella V, Buonavoglia C. Recombinant canine coronaviruses in dogs, Europe. Emerg Infect Dis. 2010; 44: 41–47. doi: 10.3201 / eid1601.090726. [PMC free article] [PubMed] [Cross Ref]
Decaro N, Buonavoglia C. An update on canine coronaviruses: viral evolution and pathobiology. Vet Microbiol. 2008; 44: 221–234. doi: 10.1016 / j.vetmic.2008.06.007. [PubMed] [Cross Ref]
Watt NJ, MacIntyre NJ, McOrist S. An extended outbreak of infectious peritonitis in a closed colony of European wildcats (Felis silvestris) J Comp Pathol. 1993; 44: 73–79. doi: 10.1016 / S0021-9975 (08) 80229-0. [PubMed] [Cross Ref]
de Groot-Mijnes JD, van Dun JM, van der Most RG, de Groot RJ. Natural history of a recurrent feline coronavirus infection and the role of cellular immunity in survival and disease. J Virol. 2005; 44: 1036–1044. doi: 10.1128 / JVI.79.2.1036-1044.2005. [PMC free article] [PubMed] [Cross Ref]
Tsai HY, Chueh LL, Lin CN, Su BL. Clinicopathological findings and disease staging of feline infectious peritonitis: 51 cases from 2003 to 2009 in Taiwan. J Feline Med Surg. 2011; 44: 74–80. doi: 10.1016 / j.jfms.2010.09.014. [PubMed] [Cross Ref]
Origin of FIP exudates. Sweat in wet FIP comes from small vessels (venules) that line the surface of the abdominal and thoracic organs (visceral) and walls (parietal), mesentery / mediastinum, and omentum. The spaces around these vessels contain a specific type of macrophages that come from monocyte progenitors that constantly recirculate between the bloodstream, the interstitial spaces around the venules, the afferent lymph, the regional lymph nodes, and back into the bloodstream. Other sites of this recirculation are located in the meninges, brain ependyma, and uveal eye tract. A small proportion of these monocytes develop into immature macrophages (monocyte / macrophage) and eventually into resident macrophages. Macrophages are constantly looking for infections.
FIPV is caused by a mutation in feline enteric coronavirus (FECV) present in lymphoid tissues and lymph nodes in the lower intestine. The mutation changes FECV cell tropism from enterocytes to peritoneal-type macrophages. Monocytes / macrophages appear to be the first cell type to be infected. This infection causes more monocytes to leave the bloodstream and begin to turn into macrophages, which continue the cycle of infection. [2]. Monocytes / macrophages do not undergo programmed cell death as usually expected, but continue to mature into large virus-loaded macrophages. These large macrophages eventually undergo programmed cell death (apoptosis) and release large amounts of virus, which then infects new monocytes / macrophages. [1]. Infected monocytes / macrophages and macrophages produce several substances (cytokines) that mediate the intensity of inflammation (disease) and immunity (resistance). [1,2].
Inflammation associated with FIP leads to three types of changes in the venules. The first is loss of vascular wall integrity, micro-bleeding, and leakage of plasma protein rich in activated complement clotting and activation factors and other inflammatory proteins. The second type of damage involves thrombosis and blocking blood flow. The third injury occurs in more chronic cases and involves fibrosis (scarring) around the blood vessels. Variations in these three events determine the amount and composition of exudates according to the four Starling forces that determine the movement of fluids between the bloodstream and interstitial spaces. [3].
The classic effusion in wet FIP is mainly due to acute damage to the vessel walls and leakage of plasma into the interstitial spaces and finally into the body cavities. Protein that escapes into the interstitial spaces attracts additional fluids, which can be exacerbated by blocking venous blood flow and increasing capillary pressure. This type of effusion, known as exudate, also contains high levels of protein, which is involved in inflammation, immune responses and blood clotting.
This fluid also contains a large number of neutrophils, macrophages / monocytes, macrophages, eosinophils and a lower number of lymphocytes and red blood cells. This classic type of fluid has the consistency of egg white and forms weak clots containing a high amount of bilirubin. Bilirubin does not originate from liver disease, but rather from the destruction of red blood cells that escape into interstitial tissue cells and are taken up by monocytes / macrophages and macrophages. Red blood cells break down and hemoglobin is broken down into heme and globin. Globin is further metabolized to biliverdin (greenish color) and finally to bilirubin (yellowish color), which is then excreted by the liver. However, cats lack the enzymes used for conjugation and are therefore ineffective in removing bilirubin from the body. [4]. This leads to the accumulation of bilirubin in the bloodstream and gives the effusion a yellow tinge. The darker the yellow tint, the more bilirubin is in the effusion, the more severe the initiating inflammatory response and the more severe the resulting bilirubinemia, bilirubinuria and jaundice.
At the opposite extreme of the classic and more acute effusion in FIP are effusions that arise predominantly from chronic infections and blockage of venous blood flow and subsequent elevation of capillary pressure. High capillary pressure results in an effusion that more closely resembles interstitial fluid than plasma, has a lower protein content, is watery rather than viscous, is clear or slightly yellow in color, is not prone to clotting, and has a lower number of acute inflammatory cells such as neutrophils. There are also FIP effusions that fall between these extremes, depending on the relative degree of acute inflammation and chronic fibrosis. These transitional types of fluid are commonly referred to in the veterinary literature as modified transudate, but this is a misnomer. Modified transudate begins as a transudate and changes as it persists and causes mild inflammation. The low-protein, low-cell effusions of FIP arise as exudates rather than transudates and do not fit this description. A more accurate term is “modified exudate” or “variant exudative effusion.”
How long do sweats usually last in cats treated with GS-441524 or GC376? The presence of abdominal effusions often leads to a large dilation of the abdomen and is confirmed by palpation, hollow needle aspiration, X-ray or ultrasound. Cats with thoracic effusions are most often presented with severe shortness of breath and are confirmed by radiological examination and aspiration. Chest effusions are almost always removed to relieve shortness of breath and recur slowly compared to abdominal effusions. Therefore, abdominal effusions are usually not removed unless they are massive and do not interfere with respiration, as they are quickly replaced. Repeated drainage of abdominal effusions can also deplete proteins and cause harmful changes in fluid and electrolyte balance in severely ill cats.
Chest effusions disappear faster with GS-441524 treatment, with improved breathing within 24-72 hours and usually disappearing in less than 7 days. Abdominal effusions usually decrease significantly within 7-14 days and disappear within 21-28 days. The detection of exudates that persist after this time depends on their amount and method of detection. Small amounts of persistent fluid can only be detected by ultrasound.
Persistence of exudates during or after antiviral treatment. There are three basic reasons for the persistence of exudates. The first is the persistence of the infection and the resulting inflammation at a certain level, which can be caused by inappropriate treatment, poor medication or drug resistance. Inadequate treatment may be the result of incorrect dosing of the wrong drug or the acquisition of virus resistance to the drug. The second reason for fluid persistence is chronic venous damage and increased capillary pressure. This may be due to a low-grade infection or residual fibrosis from an infection that has been removed. The third reason for persistence is the existence of other diseases, which can also manifest as exudates. These include congenital heart disease, in particular cardiomyopathy, chronic liver disease (acquired or congenital), hypoproteinemia (acquired or congenital) and cancer. Congenital diseases causing effusions are more common in young cats, while acquired causes and cancer are more commonly diagnosed in older cats.
Diagnosis and treatment of persistent effusions. A thorough examination of the fluid, as described above, is a prerequisite for diagnosis and treatment. If the fluid is inflammatory or semi-inflammatory and the cell pellet is positive by PCR or IHC, the reason for the persistence of the infection must be determined. Was the antiviral treatment performed correctly, was the antiviral drug active and its concentration correct, was there evidence of acquired drug resistance? If the fluid is inflammatory and PCR and IHC are negative, what other diseases are possible? Low protein and non-inflammatory fluids that are negative for PCR and IHC indicate a diagnosis of residual small vessel fibrosis and / or other contributing causes such as heart disease, chronic liver disease, hypoproteinemia (bowel disease or kidneys). Some of the disorders causing this type of effusion may require an exploratory laparotomy with a thorough examination of the abdominal organs and a selective biopsy to determine the origin of the fluid. The treatment of persistent effusions will vary greatly depending on the end cause. Persistent effusions caused by residual small vessel fibrosis in cats cured of the infection often resolve after many weeks or months. Persistent discharges caused in whole or in part by other diseases require treatment for these diseases.
Identification and characteristics of persistent effusions. The presence of fluid after 4 weeks of GS treatment is unpleasant and is usually detected in several ways depending on the amount of fluid and its location. Large amounts of fluid are usually determined by the degree of abdominal dilation, palpation, X-ray and abdominal aspiration, while smaller amounts of fluid are best detected by ultrasound. Persistent pleural effusion is usually detected by X-rays or ultrasound. Overall, ultrasound is the most accurate means of detecting and semiquantitatively determining thoracic and abdominal effusions. Ultrasound can also be used in combination with thin needle aspiration to collect small and localized amounts of fluid.
The second step in examining persistent effusions is to analyze them based on color, protein content, white and red blood cell counts, and the types of white blood cells present. Fluids generated primarily by inflammation will have protein levels close to or equal to plasma and a large number of white blood cells (neutrophils, lymphocytes, monocytes / macrophages and large vacuolated macrophages). Fluids produced by increased capillary pressure are more similar to interstitial fluid with proteins closer to 2.0 g / dl and cell counts <200. The Rivalt test is often used to diagnose FIP-related effusions. However, this is not a specific test for FIP, but rather for inflammatory effusions. It is usually positive for FIP effusions that are high in protein and cells, but is often negative for very low protein and cell effusions. The effluents that are between these two types of effusions will be tested either positively or negatively, depending on where they are in the spectrum.
The third step is the analysis of exudates for the presence of FIP virus. This usually requires 5 to 25 ml or more of fluid. For fluids with a higher protein and cell count, a smaller amount may suffice, while for fluids with a low protein and cell count, a larger amount is required. The freshly collected sample should be centrifuged and the cell pellet analyzed for the presence of viral RNA by PCR or cytocentrifuged for immunohistochemistry (IHC). The PCR test should be for FIPV 7b RNA and not for specific FIPV mutations, as the mutation test does not have sufficient sensitivity and does not provide any diagnostic benefits [5]. Samples that are positive by PCR or IHC provide definitive evidence of FIP. However, up to 30 % samples from known cases of FIP may have a false negative test either due to an inappropriate sample and its preparation, or because the RNA level of the FIP virus is below the level of detection. It is also true that the less inflammatory the fluid, the lower the virus levels. Therefore, effusions with lower protein and white blood cell levels are more likely to be tested negative because viral RNA is below the detection limit of the test.
References
[1] Watanabe R, Eckstrand C, Liu H, Pedersen NC. Characterization of peritoneal cells from cats with experimentally-induced feline infectious peritonitis (FIP) using RNA-seq. Vet Res. 2018 49 (1): 81. doi: 10.1186 / s13567-018-0578-y.
[2]. Kipar A, Meli ML, Failing K, Euler T, Gomes-Keller MA, Schwartz D, Lutz H, Reinacher M. Natural feline coronavirus infection: differences in cytokine patterns in association with the outcome of infection. Vet Immunol Immunopathol. 2006 Aug 15; 112 (3-4): 141-55. doi: 10.1016 / j.vetimm.2006.02.004. Epub
[4]. Court MH. Feline drug metabolism and disposition: pharmacokinetic evidence for species differences and molecular mechanisms. Vet Clin North Am Small Anim Pract. 2013; 43 (5): 10391054. doi: 10.1016 / j.cvsm.2013.05.002
[5]. Barker, EN, Stranieri, A, Helps, CR. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet Res 2017; 48: 60.
ABSTRACT: Acute phase proteins (APP) are proteins synthesized and released mainly by hepatocytes when cells are damaged or invaded by microorganisms. This article reviews the use of APPs in feline diseases, identifies their utility in the clinical setting, and analyzes 55 published papers. Serum amyloid A (SAA), alpha-1 acid glycoprotein (AGP), and haptoglobin are markers that the authors consider useful in monitoring the acute inflammatory response in cats. Although measurement of APP is still not routinely used in veterinary medicine, together with clinical signs and other blood parameters, they are of clinical interest and applicable in diseases such as feline infectious peritonitis, pancreatitis, renal failure, retroviral and calicivirus infections. Although there are commercially available kits for measuring feline APP, standardization of assays aimed at technical simplicity, greater species specificity, and lower associated costs will enable routine use in feline practice, as is done in the human field. keywords: inflammation, acute phase proteins, cat.
Introduction
Acute phase response (APR) is an early non-specific systemic innate immune response to a local or systemic stimulus that helps treat and restore homeostasis and minimize tissue damage when an organism is affected by trauma, infection, stress, surgery, neoplasia, or inflammation (GRUYS et al. , 2005; CRAY et al., 2009; ECKERSALL AND BELL, 2010). In this reaction, we observe several different systemic effects: fever, leukocytosis, hormonal changes - mainly cortisol and thyroxine concentrations, with secondary catabolic status and serum muscle, iron and zinc depletion (CERÓN et al. 2005, JAVARD et al. 2017). Cytokines IL-1β, TNF-α, and especially IL-6, and approximately 90 minutes after injury, increase protein synthesis in hepatocytes, lymph nodes, tonsils, and spleen, as well as blood leukocytes. These newly formed proteins are called acute phase proteins (APPs) (TIZARD, 2013b).
Acute-phase proteins
APP concentrations may increase (APP positive) or decrease (APP negative) in response to inflammation (PALTRINIERI et al., 2008) (JOHNSTON & TOBIAS, 2018). They can activate leukocytosis and complement, cause protease inhibition, lead to blood clotting and opsonization - a defense mechanism that leads to the elimination of infectious agents, tissue regeneration and restoration of health (CRAY et al., 2009). APP can have two functions, pro- and / or anti-inflammatory, which must be fine-tuned to promote homeostasis (HOCHEPIED et al., 2003).
According to the size and duration of the reaction following the stimulus, three main groups of APP are distinguished (MURATA et al., 2004; PETERSEN et al., 2004; CERÓN et al.). Positive APP can be divided into two groups: the first group includes APP with an increase of 10 up to 1000-fold in humans or 10- to 100-fold in domestic animals in the presence of inflammation - e.g. c-reactive protein (CRP) and serum amyloid A (SAA). The second group are APPs, which increase 2 to 10-fold in an inflammatory response - e.g. haptoglobin and alpha-globulins. The last group included negative APP, in which the concentration decreases in response to inflammation - e.g. albumin (KANN et al., 2012).
Acute phase positive proteins
Positive APPs are glycoproteins whose serum concentrations, when stimulated by pro-inflammatory cytokines, increase by 25 % during the disease process and are released into the bloodstream. These concentrations can be measured and used in diagnosis, prognosis, monitoring of response to treatment, as well as general health screening. They can also be considered as quantitative biomarkers of the disease, highly sensitive to inflammation but not very specific, as an increase in APP can also occur in non-inflammatory diseases (CERÓN et al., 2005; ECKERSALL and BELL, 2010).
Positive APPs respond to cytokines differently, and these groups fall into two main classes. Type 1 APP, which includes AGP, complement component 3, SAA, CRP, haptoglobin and hemopexin, is regulated by IL-1, IL-6 and TNF-α as well as glucocorticoids. Type 2, which includes three fibrinogen chains (α-, β- and γ-fibrinogen) and various inhibitory proteases, is regulated by cytokines IL-6 and glucocorticoids (BAUMANN et al., 1990; BAUMANN & GAULDIE, 1994).
In cats, the most important APP is SAA (Serum Amyloid A) or alpha-1-acid glycoprotein (AGP). The level of SAA in the blood can indicate inflammatory conditions such as feline infectious peritonitis (FIP) and other infectious diseases such as calicivirus infection, chlamydiosis, leukemia and infectious immunodeficiency, as it increases 10- to 50-fold (TIZARD, 2013b). SAA can also be elevated in other diseases such as diabetes mellitus and cancer. Haptoglobin is usually increased 2- to 10-fold and is particularly high in FIP (TIZARD, 2013b). Table 1 summarizes the individual positive APPs in the context of feline disease.
Acute phase negative proteins
The most significant negative APP is albumin, whose blood concentration decreases during APR due to amino acid aberrations towards the synthesis of positive APPs (CRAY et al., 2009; PALTRINIERI, 2007a). Other negative APPs are transferrin, transthyretin, retinol ligand, and cortisol binding protein, proteins involved in vitamin and hormone transport (JAIN et al., 2011).
Acute phase proteins in cat disease
Unlike cytokines, which are small in size and rapidly filtered by the kidney, acute phase proteins have a higher molecular weight (greater than 45 kDa) and consequently remain in plasma for longer (SALGADO et al., 2011).
APP levels can only indicate inflammation, and consequently their concentrations can help diagnose and monitor the disease. APP can help detect subclinical inflammation, distinguish acute from chronic disease, and predict its course (VILHENA et al, 2018; JAVARD et al., 2017). Because APRs begin before specific immunological changes occur, they can be used as an early marker of disease before leukogram changes occur, with their magnitude related to disease severity (PETERSEN et al., 2004; CÉRON et al., 2005; VILHENA et al., 2005). , 2018). For this reason, disease monitoring can be considered one of the most interesting and promising applications of APP.
APP levels along with clinical signs and blood tests have been evaluated in a variety of animal diseases (ie, FIP, canine inflammatory disease, leishmaniasis, ehrlichiosis, and canine pyometra) and have been shown to be useful in diagnosis, response to treatment, and prognosis (ECKERSALL et al. ), 2001; MARTINEZ-SUBIELA et al., 2005; SHIMADA et al., 2002; JERGENS et al., 2003; GIORDANO et al., 2004; PETERSEN et al., 2004; DABROWSKI et al., 2009; VILHENA et al., 2018).
To obtain complete information on APR, one major and one moderate positive as well as one negative APP should be evaluated simultaneously (CERÓN et al., 2008). High concentrations of major APP are usually associated with infectious diseases, usually systemic bacterial infection or immune-mediated disease (CERÓN et al., 2008; TROÌA et al., 2017). Although APPs should be analyzed along with white blood cell and neutrophil counts, they are most sensitive in the early detection of inflammation and infection (CERÓN et al., 2008; ALVES et al., 2010). However, the specificity of these proteins is low in determining the cause of the process, and also increases in physiological conditions such as pregnancy (PALTRINIERI et al., 2008).
APP
The disease
SAA
FIP Induced inflammation and surgery Various diseases (pancreatitis, renal failure, FLUTD, tumors, diabetes mellitus; kidney disease, injury, etc.) Sepsis FeLV; hemotropic mycoplasma infections Hepatozoonfelis and Babesia vogeli infection Dirofilariaimmitis FIV cats treated with recombinant feline interferon
AGP
Chlamydophila psittaci infection; Pancreatitis and pancreatic tumors FIP Lymphoma and other tumors Induced inflammation and surgery FIV cats treated with recombinant feline interferon Abscesses, pyothorax, adipose tissue necrosis Various diseases (FLUTD, tumors, diabetes mellitus, kidney diseases, injuries, etc.)
Haptoglobin
FIP Induced inflammation and surgery Abscesses, pyothorax, adipose tissue necrosis Various diseases (FLUTD, tumors, diabetes mellitus, kidney diseases, injuries, etc.) Hepatozoonfelis and Babesia vogeli infection FeLV, hemotropic mycoplasmas Dirofilariaimmitis
CRP
FIV cats treated with recombinant feline interferon Induced inflammation and surgery
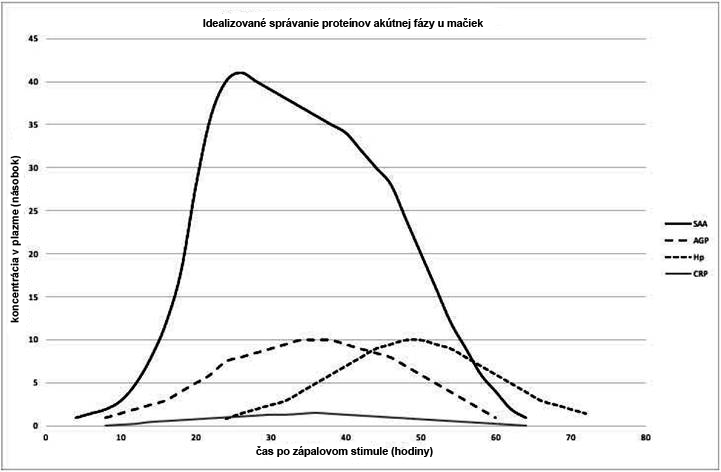
Figure 1 shows the expected behavior of acute phase positive proteins based on revised studies. AGP, SAA and haptoglobin have been identified as useful indicators for monitoring the acute inflammatory response in cats (WINKEL et al., 2015; PALTRINIERI et al., 2007a, b; KAJIKAWA et al., 1999). APPs in cats were first identified after comparative measurements in the serum of clinically normal and diseased animals, in experimentally induced inflammation studies, and in postoperative studies (KAJIKAWA et al., 1999). The concentration of SAA reportedly increased first, followed by an increase in AGP and haptoglobin, in contrast to a less pronounced increase in CRP (KAJIKAWA et al., 1999). One study showed that CRP behaves similarly to SAA and AGP in cat inflammation (LEAL et al., 2014).
Serum Amyloid A
SAA is one of the major APPs in several species, important in both humans and cats (KAJIKAWA et al., 1999). It modulates the immune response by attracting inflammatory cells to tissues and leading to the production of multiple inflammatory cytokines (GRUYS et al., 2005; TIZARD, 2013a). Its concentration can increase more than 1,000 times in an inflammatory condition, which we then understand as inflammation (TAMAMOTO et al., 2013). However, such an increase can be observed in both non-inflammatory and inflammatory diseases and neoplasms (TAMAMOTO et al., 2013). According to a study in cats that underwent surgery, SAA levels begin to increase approximately 3 to 6 hours, peaking 21 to 24 hours after surgery (SASAKI et al., 2003).
Figure 1 - Idealized behavior of acute phase proteins in cats after inflammatory stimuli. The values representing the changes cannot be considered absolute. Increase in serum amyloid A (SAA) 3 to 6 h after challenge, peak at 21 to 24 h, peak size 10 to 50 times its basal plasma concentration. Alpha 1 acid glycoprotein (AGP) increases 8 h after challenge, peak at 36 h, size at peak time 2 to 10 times its baseline plasma concentration. Haptoglobulin (Hp) increase 24 h after challenge, peak 36 to 48 h, peak size 2 to 10 times its basal plasma concentration. C-reactive protein (CRP) increased 8 h after challenge, peak at 36 h, peak size 1.5 times its basal values.
Alpha 1-acid glycoprotein
Alpha 1-acid glycoprotein (AGP) is an acute phase-reactive protein found in the serum mucoid portion of serum (SELTING et al., 2000; WINKEL et al., 2015). Like most positive APPs, AGP is a glycoprotein synthesized predominantly by hepatocytes in APR and released into the bloodstream (CÉRON et al., 2005).
AGP can be used to monitor early interferon treatment in cats infected with feline immunodeficiency virus (FIV) (GIL et al., 2014). AGP as well as haptoglobin (Hp) are increased in anemic cats suffering from pyothorax, abscesses or fat necrosis (OTTENJANN et al., 2006).
Changes in AGP in feline neoplasia do not appear to be consistent across studies. Some of them do not describe any changes in cats with lymphoma (CORREA et al., 2001). Others point to an increase in both AGP and SAA in cats with sarcomas, carcinomas, or other round cell tumors (SELTING et al., 2000; TAMAMOTO et al., 2013; MEACHEN et al., 2015; HAZUCHOVA et al., 2017).
AGP is important as an indicator test for FIP, which is used specifically in Europe (CECILIANI et al., 2004). GIORI et al. examined the specificity and sensitivity of several tests in 12 cats, with 33.33 % cats being FIP negative based on histopathology and immunohistochemistry and 66.66 % cats being FIP positive confirmed by histopathology and immunohistochemistry. This author concludes that immunohistochemistry must always be performed to confirm FIP, but high concentrations of AGP can help support the diagnosis of FIP if immunohistochemistry cannot be performed and histopathology is not convincing.
Haptoglobin
Haptoglobin (Hp) is one of the most important acute phase proteins in cattle, sheep, goats, horses and cats (TIZARD, 2013a), synthesized mainly by hepatocytes but also by other tissues such as skin, lungs and kidneys (JAIN et al, 2011 ). Hp binds to iron molecules and makes them inaccessible to invasive bacteria, thereby inhibiting bacterial proliferation and invasion. Subsequently, it also binds to free hemoglobin, thus preventing its oxidation with lipids and proteins (TIZARD, 2013a), which justifies a reduction in Hp in case of hemolysis.
In cats, Hp usually increases 2- to 10-fold in inflammatory conditions, and is particularly high in FIP (TIZARD, 2013a). However, both Hp and SAA did not provide sufficient support to distinguish FIP from other causes of effusion compared to AGP (HAZUCHOVÁ et al., 2017).
Measurement APP
The serum is composed of a large number of individual proteins in which the detection of changes in its fractions can provide important diagnostic information (ECKERSALL, 2008).
Ideally, measurement of all serum proteins should be available so that they can be used as a diagnostic tool in relation to inflammatory diseases. Currently, APPs (Table 2) can be determined by enzyme-linked immunosorbent assay (ELISA), radioimmunoassay, nephelometry, immunoturbidimetry (IT), Western blot, and messenger ribonucleic acid (mRNA) analysis (CÉRON et al., 2005; PALTRINIERI et al., 2008; SCHREIBER et al., 1989). Although some human APP tests have been automated for veterinary medicine, species-specific tests are still limited. Cross-species differences in APP and the limited availability of cross-reactive agents have so far contributed to the low routine level of APP determination in veterinary laboratories, especially in cats. Regardless, the technology is evolving and routine monitoring of clinically relevant APPs in cats can be expected in the near future.
Conclusion
Acute phase proteins in cats are biomarkers suitable for monitoring inflammation, along with other clinical and laboratory findings that are useful in diagnosing subclinical changes, monitoring the development and effect of the disease in the body, as well as in evaluating the response to treatment.
In cats, SAA APP, which is most pronounced in response to inflammation, is followed by AGP and haptoglobin, in contrast to CRP, which is used in other species.
Although there are commercially available kits for determining feline APPs, standardization of tests for technical simplicity, higher species specificity with lower associated costs will allow routine use in feline practice, as is done in human medicine.
Analyzes
Pros
Cons
Radioimmunoassay
24 to 48 hours to obtain results, specific operator skills required
ELISA
Commercially available species-specific kits
Lack of automation, expensive, some "between-run" inaccuracy
Immunoturbidimetry
30 minutes to obtain results, customizable with a biochemical analyzer
Western Blot
Long time for immunoblot processing
Nephelometric immunoassays
They depend on the cross-reactivity of the increased antiserum
Table 2 - Advantages and disadvantages of possible APP measurement techniques.
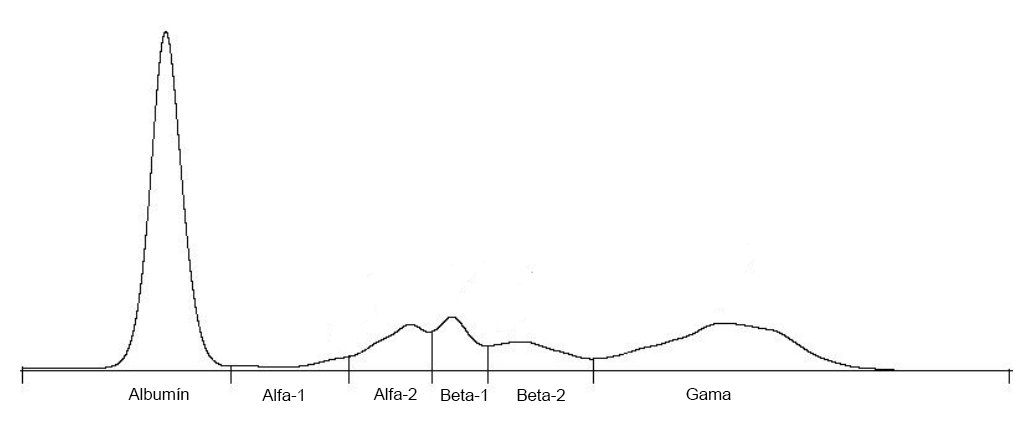
Appendix: APP and their position in the electrophoretogram
Although there are tests directly for a specific APP, it is useful to know in which region the electrophoretograms are located.
Electrophoretogram demonstration (Serum protein electrophoresis output)
Serum protein
Electrophoretic region
α1-acid glycoprotein
α1 (alpha-1)
Serum Amyloid A
α (alpha)
Haptoglobin
α2 (alpha-2)
Ceruloplasmin
α2 (alpha-2)
Transferrin
β1 (beta-1)
C-reactive protein
γ (gamma)
Position of serum proteins in electrophoretogram
References
ALVES, AE et al. Leucogram and serum acute phase protein concentrations in queens submitted to conventional or videolaparoscopic ovariectomy. Arquivo Brasileiro de Medicina Veterina- ria e Zootecnia, v.62, n.1, p.86-91, 2010. Available from:. Accessed: Oct. 10, 2018. doi: 10.1590 / S0102-09352010000100012.
BAUMANN, H. & GAULDIE, J. The acute phase response. Immunol Today, v.15, n.2, p.74-80, 1994. Available from: https://doi.org/10.1016/0167-5699(94)90137-6. Accessed: Aug. 21, 2018. doi: 10.1016 / 0167-5699 (94) 90137-6.
BAUMANN, H. et al. Distinct regulation of the interleukin-1 and interleukin-6 response elements of the rat haptoglobin gene in rat and human hepatoma cells. Molecular and Cellular Biology, v.10, n.11, p.5967–5976, 1990. Available from: Accessed: Aug. 21, 2018. doi: 10.1128 / MCB.10.11.5967.
BENCE, L. et al. An immunoturbidimetric assay for rapid quantitative measurement of feline alpha-1-acid glycoprotein in serum and peritoneal fluid. Veterinary Clinical Pathology, v.34, n.4, p335-341, 2005. Available from:. Accessed: Jan. 13, 2019. doi: 10.1111 / j.1939-165X.2005.tb00058.x.
CALLAHAN, G. & YATES, R. Veterinary Clinical Laboratory Immunology. In Warren, A. Basic Veterinary Immunology, pp. 295-317, 2014. Boulder, Colorado: University Press of Colorado.
CECILIANI, F. et al. Decreased sialylation of the acute phase protein α1-acid glycoprotein in feline infectious peritonitis (FIP). Veterinary Immunology and Immunopathology, v.99, n.3- 4, p.229-236, 2004. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j. vetimm.2004.02.003.
CERON, J. et al. Acute phase proteins in dogs and cats: current knowledge and future perspectives. Veterinary Clinical
Pathology, v.34, n.2, p.85-99, 2005. Available from:. Accessed: Aug. 20, 2018. doi: 10.1111 / j.1939-165X.2005.tb00019.x.
CERÓN, JJ A seven-point plan for acute phase protein interpretation in companion animals. Veterinary Journal, v.177, n.1, p.6-7, 2008. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / j. tvjl.2007.12.001.
CORREA, SS et al. Serum alpha 1-acid glycoprotein concentration in cats with lymphoma. Journal of the American Animal Hospital Association, v.37, n.2, p.153-158, 2001. Available from: https://doi.org/10.5326/15473317-37-2-153. Accessed: Aug. 24, 2018. doi: 10.5326 / 15473317-37-2-153.
CRAY, C. et al. AcutePhase Response in Animals: A Review. Comparative Medicine, v.59, n.6, p.517–526, 2009. Available from:. Accessed: Aug. 21, 2018.
DABROWSKI, R. et al. Usefulness of C-reactive protein, serum amyloid A component and haptoglobin determinations in bitches with pyometra for monitoring early postovariohysterectomy complications. Theriogenology, v.72, n.4, p.471–476, 2009. Available from:. Accessed: Aug. 23, 2018. doi: 10.1016 / j.theriogenology.2009.03.017.
DUTHIE, S. et al. Value of α1-acid glycoprotein in the diagnosis of feline infectious peritonitis. The Veterinary Record, v.141, n.12, p.299–303, 1997. Available from:. Accessed: Aug. 11, 2018. doi: 10.1136 / vr.141.12.299.
ECKERSALL, P. Proteins, Proteomics, and the Dysproteinemias. In Kaneko, J., Harvey, J. & Bruss, M. In Clinical Biochemistry of Domestic Animals. 6th ed. USA: Elsevier, 2008, Chap. 5, pp.117-155.
ECKERSALL, PD & BELL, R. Acute phase proteins: Biomarkers of infection and inflammation in veterinary medicine. The Veterinary Journal, v.185, n.1, p.23-27, 2010. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / j.tvjl.2010.04.009.
ECKERSALL, PD et al. Acute phase protein response in an experimental model of ovine caseous lymphadenitis. BMC Veterinary Research, v.19, p.3-35, 2007. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2010.04.009.
ECKERSALL, PD et al. Acute phase proteins in serum and milk from dairy cows with clinical mastitis. Veterinary Record, v.148, n.2, p.35–41, 2001. Available from:. Accessed: Aug. 22, 2018. doi: 10.1136 / vr.148.2.35.
GIL, S. et al. Oral recombinant feline interferon-omega as an alternative immune modulation therapy in FIV positive cats: Clinical and laboratory evaluation. Research in Veterinary Science, v.96, n.1, p.79–85, 2014. Available from:. Accessed: Oct. 10, 2018. doi: 10.1016 / j.rvsc.2013.11.007.
GIORDANO, A. et al. Changes in some acute phase protein and immunoglobulin concentrations in cats affected by feline infectious peritonitis or exposed to feline coronavirus infection. The Veterinary Journal, v.167, n.1, p.38-44, 2004. Available from: https://doi.org/10.1016/S1090-0233(03)00055-8. Accessed: Aug. 9, 2018. doi: 10.1016 / S1090-0233 (03) 00055-8.
GIORI, L. et al. Performances of different diagnostic tests for feline infectious peritonitis in challenging clinical cases. Journal of Small Animal Practice, v.52, n.3, p.152-157, 2011. Available from: https://doi.org/10.1111/j.1748-5827.2011.01042.x. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1748-5827.2011.01042.x.
GRUYS, E. et al. Acute phase reaction and acute phase proteins. Journal of Zhejiang University. Science B, v.6, n.11, p.1045- 1056, 2005. Available from:. Accessed: Aug. 21, 2018. doi: 10.1631 / jzus.2005.B1045.
HAZUCHOVA, K. et al. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. Journal of Feline Medicine and Surgery, v.19, n.8, p.809-816, 2017. Available from: https://doi.org/10.1177/1098612X16658925. Accessed: Aug. 11, 2018. doi: 10.1177 / 1098612X16658925.
HOCHEPIED, T. et al. α1-Acid glycoprotein: an acute phase protein with inflammatory and immunomodulating properties. Cytokine Growth Factor Rev, v.14, n.1, p.25–34, 2003. Available from: https://doi.org/10.1016/S1359-6101(02)00054-0. Accessed: Aug. 21, 2018. doi: 10.1016 / S1359-6101 (02) 00054-0.
JACOBSEN, S. et al. Evaluation of a commercially available human serum amyloid A (SAA) turbidometric immunoassay for determination of equine SAA concentrations. Veterinary Journal, v.172, n.2, p.315–319, 2006. Available from:. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2005.04.021.
JAIN, S. et al. Acute-phase proteins: As diagnostic tool. Journal of Pharmacy and Bioallied Sciences, v.3 v.1, p.118–127, 2011. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3053509/. Accessed: Aug. 21, 2018. doi: 10.4103 / 0975-7406.76489.
JAVARD R. et al. Acute phase proteins and iron status in cats with chronic kidney Disease. Journal of Veterinary Internal Medicine, v.31, n.2, p.457-464, 2017. Available from:. Accessed: Oct. 10, 2018. doi: 10.1111 / jvim.14661.
JERGENS, AE et al. A scoring index for disease activity in canine inflammatory bowel disease. Journal of Veterinary Internal Medicine, v.17, n.3, p.291–297, 2003. Available from:. Accessed: Aug. 22, 2018. doi: 10.1111 / j.1939-1676.2003.tb02450.x.
KAJIKAWA, T. et al. Changes in concentrations of serum amyloid A protein, alpha 1-acid glycoprotein, haptoglobin, and C-reactive protein in feline sera due to induced inflammation and surgery. Veterinary Immunology and Immunopathology, v.68, n.1, p. 91-98, 1999. Available from: Accessed: Aug. 10, 2018. doi: 10.1016/S0165-2427(99)00012-4.
KANN, R. et al. Acute phase proteins in healthy and sick cats. Research in Veterinay Science, v.93, n.2. p.649-654, 2012. Available from: https://doi.org/10.1016/j.rvsc.2011.11.007. Accessed: Aug. 20, 2018. doi: 10.1016 / j.rvsc.2011.11.007.
KURIBAYASHI, T. et al. Alpha 1-acid glycoprotein (AAG) levels in healthy and pregnant beagle dogs. Experimental Animals, v.52, n. 5, p.377–381, 2003. Available from:. Accessed: Jan. 13, 2019. doi: 10.1538 / expanim.52.377.
LEAL, R. et al. Monitoring acute phase proteins in retrovirus infected cats undergoing feline interferon-ω therapy. Journal of Small Animal Practice, v.55, n.1, p.39-45, 2014. Available from: https://doi.org/10.1111/jsap.12160. Accessed: Jan. 6, 2019. doi: 10.1111 / jsap.12160.
MARTÍNEZ-SUBIELA, S. et al. Analytical validation of commercial techniques for haptoglobin determination, C reactive protein and amiloid A series in canines [Analytical validation of commercial techniques for haptoglobin, C reactive protein and serum amyloid A determinations in dogs]. Archivos de Medicina Veterinaria, v.37, n.1, 2005. Available from:. Accessed: Jan. 13, 2019. doi: 10.4067 / S0301-732X2005000100009.
MEACHEM, MD et al. A comparative proteomic study of plasma in feline pancreatitis and pancreatic carcinoma using 2-dimensional gel electrophoresis to identify diagnostic biomarkers: A pilot study. Canadian Journal of Veterinary Research, v.79, n.3, p.184-189, 2015. Available from:. Accessed: Oct. 10, 2018.
MURATA, H. et al. Current research on acute phase proteins in veterinary diagnosis: An overview. The Veterinary Journal, v.168, n.1, p.28–40, 2004. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / S1090-0233 (03) 00119-9.
OTTENJANN, M. et al. Characterization of the anemia of inflammatory disease in cats with abscesses, pyothorax, or fat necrosis. Journal of Veterinary Internal Medicine, v.2, n.5, p. 1143-1150, 2006. Available from:. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1939-1676.2006.tb00713.x.
PALTRINIERI, S. Early biomarkers of inflammation in dogs and cats: The acute phase protein. Veterinary Research Communications, v.31, n.1, p.125-129, 2007a. Available from: . Accessed: Aug. 21, 2018. doi: 10.1007 / s11259-007-0107-3.
PALTRINIERI, S. et al. Serum alpha1-acid glycoprotein (AGP) concentration in non-symptomatic cats with feline coronavirus (FCoV) infection. Journal of Feline Medicine and Surgery, v.9, n.4, p.271-277, 2007b. Available from:. Accessed: Aug. 11, 2018. doi: 10.1016 / j. jfms.2007.01.002.
PALTRINIERI, S. The feline acute phase reaction. Review. The Veterinary Journal, v.111, n.1, p.26-35, 2008. Available from: https://doi.org/10.1016/j.tvjl.2007.06.005. Accessed: Aug. 24, 2018. doi: 10.1016 / j.tvjl.2007.06.005.
PETERSEN, H. et al. Application of acute phase protein measurements in veterinary clinical chemistry. Veterinary Research, v.35, n.2, p.163–187, 2004. Available from:. Accessed: Aug. 20, 2018. doi: 10.1051 / vetres: 2004002.
SALGADO, FJ, et al. (2011). Acute phase proteins as biomarkers of disease: from Bench to Clinical Practice. In Veas, F. Acute Phase Proteins as Early Non-Specific Biomarkers of Human and Veterinary Diseases. Rijeka, Croatia: InTech. Available from: http://www.documentation.ird.fr/hor/fdi:010060045. Accessed: Aug. 21, 2018. doi: 10.5772 / 1045.
SASAKI, K. et al. Evaluation of feline serum amyloid A (SAA) as an inflammatory marker. Journal of Veterinary Medical Science, v.65, n.4, p.545-8, 2003. Available from:. Accessed: Aug. 10, 2018.
SCHREIBER, G. et al. The acute phase response in the rodent. Annals of the New York Academy of Science, v.557, p.61–85, 1989. Available from:. Accessed: Aug. 24, 2018. doi: 10.1111 / j.1749- 6632.1989.tb24000.x.
SELTING, K. et al. Serum alpha 1-acid glycoprotein concentrations in healthy and tumor-bearing cats. Journal of Veterinary Internal Medicine, v.14, n.5, p.503-506, 2000. Available from:. Accessed: Aug. 9, 2018. doi: 10.1111 / j.1939-1676.2000.tb02267.x.
SHIMADA, T. et al. Monitoring C-reactive protein in beagle dogs experimentally inoculated with Ehrlichiacanis. Veterinary Research Communications, v.26, n.3, p.171–177, 2002. Available from:. Accessed: Aug. 22, 2018. doi: 10.1023 / A: 1015290903332.
SILVESTRE-FERREIRA, AC et al. Serum acute phase proteins in Dirofilariaimmitis and Wolbachia seropositive cats. Journal of Feline Medicine and Surgery, v.19, n.6, p.693–696, 2017. Available from: https://doi.org/10.1177/1098612X15625435. Accessed: Sep. 16, 2018. doi: 10.1177 / 1098612X15625435.
TAMAMOTO, T. et al. Serum amyloid A as a prognostic marker in cats with various diseases. Journal of Veterinary Diagnostic Investigation, v.25, n.3, p.428–432, 2013. Available from:. Accessed: Jan. 27, 2019.
TECLES, F. et al. Validation of a commercially available human immunoturbidimetric assay for haptoglobin determination in canine serum samples. Veterinary Research Communications, v.31, n.1, p.23–36, 2007. Available from:. Accessed: Jan. 13, 2019. doi: 10.1007 / s11259-006-3397-y.
TERWEE, J. et al. Characterization of the systemic disease and ocular signs induced by experimental infection with Chlamydia psittaci in cats. Veterinary Microbiology, v.59, 259-281, 1998. Available from:. Accessed: Aug. 20, 2018. doi: 10.1016 / S0378-1135 (97) 00185-5.
TIZARD, I. Innate immunity: proinflammatory and antimicrobial mediators / systemic responses to inflammation. In Veterinary Immunology. 9.ed. St. Louis, Missouri: Saunders, Elsevier, 2013a. Chap. 6, pp.52-58.
TIZARD, I. Innate immunity: proinflammatory and Atimicrobial mediators / systemic responses to Inflammation. In Veterinary Immunology. 9.ed. St. Louis, Missouri: Saunders, Elsevier, 2013b. Chap. 4, pp.31-40.
TROÌA, R. et al. Serum amyloid A in the diagnosis of feline sepsis. Journal of Veterinary Diagnostic Investigation, v.29, n.6, p.856-859, 2017. Available from:. Accessed: Aug. 11, 2018. doi: 10.1177 / 1040638717722815.
VILHENA, H. et al. Acute phase proteins response in cats naturally infected by hemotropic mycoplasmas. Comparative Immunology, Microbiology & Infectious Diseases, v.56, p.1-5, 2018. Available from: https://doi.org/10.1016/j.cimid.2017.11.001. Accessed: Aug. 11, 2018. doi: 10.1016 / j.cimid.2017.11.001.
VILHENA, H. et al. Acute phase proteins response in cats naturally infected with Hepatozoonfelis and Babesia vogeli. Veterinary Clinical Pathology, v.48, n.1, p.72-76, 2017. Available from: https://doi.org/10.1111/vcp.12451. Accessed: Aug. 10, 2018. doi: 10.1111 / vcp.12451.
WEIDMEYER, C. & SOLTER, P. Validation of human haptoglobin immunoturbidimetric detection of haptoglobin in equine and canine serum and plasma. Veterinary Clinical Pathology, v.24, n.4, p.141–146, 1996. Available from:. Accessed: Jan. 13, 2019. doi: 10.1111 / j.1939-165X.1996.tb00988.x.
WHICHER, T. et al. Immunonephelometric and immunoturbidimetric assays for proteins. Critical Reviews in Clinical Laboratory Sciences, v.18, n.3, p.213–260, 1983. Available from: https://doi.org/10.3109/10408368209085072. Accessed: Aug. 13, 2019. doi: 10.3109 / 10408368209085072.
WINKEL, V. et al. Serum α-1 acid glycoprotein and serum amyloid A concentrations in cats receiving antineoplastic treatment for lymphoma. American Journal Veterinary Research, n.76, v.11, p.983-988, 2015. Available from:. Accessed: Aug. 22, 2018. doi: 10.2460 / ajvr.76.11.983.
Abbreviations: SC - subcutaneous IV - intravenous IM - to the muscle PO - per os - orally SID - once a day BID - 2x this q24h - once every 24 hours q12h - once in 12 hours
Introduction
Antiviral resistance is well documented in diseases such as HIV / AIDS and hepatitis C. In some cases, this resistance is present in the infecting virus, but is more often due to long-term drug exposure. Resistance to GC376 [1] and GS-441524 [2] has also been documented in cats with naturally acquired FIP. Resistance develops based on mutations in regions of the viral genome that contain targets for the antiviral drug. For example, several amino acid changes (N25S, A252S or K260N) were detected in the GIP376-resistant FIPV isolate (3CLpro). [3]. A change in N25S in 3CLpro was found to cause a 1.68-fold increase in 50 % GC376 inhibitory concentration in tissue cultures [3]. Resistance to GC376, although recognized in initial field trials, has not yet been described. GC376 is less popular in the treatment of FIP and is not recommended for cats with ocular or neurological FIP. [1].
Natural resistance to GS-441524 was observed in one of 31 cats treated for naturally occurring FIP [2]. One of the 31 cats in the original GS-441524 field study also appeared to be resistant, as viral RNA levels did not decrease throughout the treatment period and the symptoms of the disease did not abate. Although this virus has not been studied, resistance to GS-5734 (Remdesivir), a prodrug of GS-441524, has been established in tissue culture by amino acid mutations in RNA polymerase and corrective exonuclease. [4].
Resistance to GS-441524 has been confirmed in a number of cats that have been treated for FIP with GS-441524 in the last 3 years, especially among cats with neurological FIP [5]. Resistance to GS441524 is usually partial and higher doses often cure the infection or significantly reduce the symptoms of the disease during treatment. Interestingly, resistance to GS-441524 has also been found in patients with Covid19 treated with Remdesivir [12]. An immunocompromised patient developed a prolonged course of SARS-CoV-2 infection. Remdesivirus treatment initially alleviated symptoms and significantly reduced virus levels, but the disease returned with a large increase in virus replication. Whole genome sequencing identified an E802D mutation in nsp12 RNA-dependent RNA polymerase that was not present in pre-treatment samples and caused a 6-fold increase in resistance.
Although the history of molnupiravir and its recent use in the treatment of FIP has been described [6], there are currently no studies documenting natural or acquired resistance to molnupiravir. Molnupiravir has been shown to function as an RNA mutagen causing several defects in the viral genome [7]while remdesivir / GS-441524 is a non-binding RNA chain terminator [8], which suggests that its resistance profile will be different.
Overcoming resistance to GS-441524
Drug resistance can only be overcome in two ways: 1) by gradually increasing the dose of the antiviral to achieve drug levels in body fluids that exceed the resistance level, or 2) by using another antiviral that has a different mechanism of resistance, either alone or in combination. So far, the first option has been chosen, which has proved effective in many cases. However, resistance to GS-441524 may be complete or so high that increasing the dose is no longer effective. In such cases, the second option is increasingly used. Currently available alternatives to GS-441524, although still from an unapproved market, are GC376 and molnupiravir.
Antiviral drug treatment regimens for resistance to GS-441524
GC376 / GS-441524
The combined GS / GC regimen has been shown to be effective in cats treated with GS-441524 at doses up to 40 mg / kg without cure due to resistance to GS-441524. It is better to intervene as soon as resistance to GS-441524 is detected, which will allow the cat to be cured sooner and at lesser cost to the owner.
Rainman is the current supplier of GC376, which comes in 4 ml vials at a concentration of 53 mg / ml.
GS / GC dosage: The dose of GS (SC or PO equivalent) in combination antiviral therapy is the same as the dose needed to adequately control the symptoms of the disease. This is usually the last dose used before the end of treatment and relapse. To this dose of GS-441524, GC376 is added at a dose of 20 mg / kg SC q24h regardless of the form of FIP. This is sufficient for most cats, including many cats with neuro FIP, but some will need higher doses. If remission of clinical signs is not achieved or blood tests are of concern, the dose of GC376 is increased by 10 mg / kg up to 50 mg / kg SC q24h.
Duration of treatment: An eight-week combination GC / GS treatment is recommended, which is added to previous GS monotherapy. Some cats were cured at 6 weeks of combination therapy, but relapse is more likely than at 8 weeks.
Side effects: Most cats have no serious side effects. However, about one in five cats may experience nausea or discomfort at the beginning of treatment and sometimes longer. These side effects do not appear to be dose dependent and can be treated with anti-nausea drugs such as Cerenia, Ondansetron or Famotidine. Ondansetron appears to have performed better in some cats.
Molnupiravir
Molnupiravir has been reported to be effective in monotherapy in cats with FIP by at least one Chinese retailer GS-441524 [9], but there are no reports of its use in cats with resistance to GS-441524. However, resistance to GS-441524 is unlikely to spread to molnupiravir. The fact that it has been found to be effective as an oral medicine also makes it attractive for treatment alone, as many cats resistant to GS-441524 have suffered from injections for a very long time.
A field study of molnupiravir reportedly consisted of 286 cats with various forms of naturally occurring FIP, which were examined in pet clinics in the United States, the United Kingdom, Italy, Germany, France, Japan, Romania, Turkey and China. Among the 286 cats that participated in the trial, no deaths occurred, including seven cats with ocular (n = 2) and neurological (n = 5) FIP. Twenty-eight of these cats were cured after 4-6 weeks of treatment and 258 after 8 weeks. All treated cats remained healthy 3-5 months later, a period during which cats that were not successfully cured would be expected to relapse. These data provide convincing evidence of the safety and efficacy of molnupiravir in cats with various forms of FIP. However, we hope that this field study will be written in the form of a manuscript, submitted for review and published. Nevertheless, it is now sold to cat owners with FIP. At least one other major retailer of GS-441524 is also interested in using molnupiravir for FIP, indicating a demand for further treatment of cats with FIP antivirals.
Molnupiravir dosage: The safe and effective dosing of molnupiravir in cats with FIP has not been established based on closely controlled and monitored field studies such as those performed for GC376 [1] and GS-441524. [2]. However, at least one seller from China in his flyer for a product called Hero-2801 [9] provided some pharmacokinetic and field trial data for Molnuparivir in cats with naturally occurring FIP. This information does not clearly state the amount of molnuparivir in one of their “50 mg tablets” and the actual dosing interval (q12h or q24h?). The dose used in this study also seemed too high. Fortunately, an estimated starting dose of molnuparivir in cats with FIP can be obtained from the published studies of EIDD-1931 and EIDD-2801 [15] in vitro on cell cultures and laboratory and field studies GS-441524 [14,18]. Molnupiravir (EIDD-2801) has an EC50 of 0.4 μM / μl against FIPV in cell culture, while the EC50 of GS-441524 is approximately 1.0 μM / μl. [18]. Both have a similar oral absorption of approximately 40-50 %, so an effective subcutaneous (SC) dose of molnupiravir would be approximately half the recommended starting dose of 4 mg / kg SC q24h for GS441524. [14] or 2 mg / kg SC q24h. The oral (PO) dose would be doubled to account for less effective oral absorption per 4 mg / kg PO q24h dose. The estimated initial effective oral dose of molnupiravir in cats with FIP can also be calculated from the available Covid-19 treatment data. Patients treated with Covid-19 are given 200 mg of molnupiravir PO q12h for 5 days. This dose was, of course, calculated from a pharmacokinetic study performed in humans, and if the average person weighs 60-80 kg (70 kg), the effective inhibitory dose is 3,03.0 mg / kg PO q12h. The cat has a basal metabolic rate 1.5-fold higher than humans, and assuming the same oral absorption in both humans and cats, the minimum dose for cats according to this calculation would be 4.5 mg / kg PO q12h in neocular and non-neurological forms of FIP. If molnupiravir crosses the blood-brain and blood-brain barriers with the same efficacy as GS-441524 [3,18], the dose should be increased to 1,51.5 and 2,02.0-fold to ensure adequate penetration into aqueous humor and cerebrospinal fluid for ocular cats (88 mg / kg PO, q12 h), respectively. neurological FIP (~ 10 mg / kg PO, q12 h). These doses are comparable to those used in ferrets, where 7 mg / kg q12h maintains sterilizing blood levels of the influenza virus drug (1.86 μM) for 24 hours. [10]. Doses in ferrets of 128 mg / kg PO q12h caused almost toxic blood levels, while a dose of 20 mg / kg PO q12h caused only slightly higher blood levels. [10].
Molnupiravir / GC376 or Molnupiravir / GS-441524
Combinations of molnupiravir with GC376 or GS-441524 will be used more and more frequently, not only to synergy or complement their individual antiviral effects, but also as a way to prevent drug resistance. Medicinal cocktails have been very effective in preventing drug resistance in HIV / AIDS patients [11]. However, there is currently insufficient evidence on the safety and efficacy of the combination of molnupiravir with GC376 or GS-441524 as initial treatment for FIP.
Case studies
Rocky - DSH MN Neuro FIP
A 9-month-old neutered domestic shorthair cat obtained as a rescue kitten had several weeks of seizures with increasing frequency, ataxia and progressive paresis. The blood tests were unremarkable. FIP treatment was started at a dose of 15 mg / kg BID GS-441524, which decreased to SID for about a week. The cat showed improvement, seizures stopped, and mobility increased within 24 hours of starting treatment. Within 5 days of treatment, the cat was able to move again. However, approximately 2 weeks after the start of treatment, the cat experienced loss of vision, decreased mobility, recovery of seizures and difficulty swallowing. Dose adjustments of levetiracetam and prednisolone were made, as well as a change in the composition of GS-441524, followed by a temporary improvement in motility and swallowing and a reduction in seizures, but overall the cat's condition worsened. The dose of GS-441524 was gradually increased to 25 mg / kg, with little or no improvement. At this point, GS was taken orally at a dose of 25 mg / kg (estimated to be approximately 12.5 mg / kg) and within 3 days, the cat began to move, improved vision, and stopped seizures with increased energy and appetite. Improvement in cats continued for approximately 4 weeks with oral administration of GS-441524, then stopped for approximately 3 weeks before rapidly progressing paresis. Oral doses up to 30 mg / kg SC equivalent have been tested but have no effect. GS-441524 was then injected at a dose of 20 mg / kg and the cat was able to move again within 4 days with good appetite and energy. After 2 weeks, a dose of GC376 20 mg / kg BID was added to the dosing regimen. The cat terminated 6 weeks of the GS441524 and GC376 combination therapy and then discontinued the treatment. Although the cat has certain permanent neurological deficits, its condition is stable, it has good mobility, appetite and activity for 9 months after the end of antiviral treatment.
A four-month-old neutered domestic shorthair cat obtained as a rescue kitten was presented with a monthly history of lethargy and a progressive history of ataxia, hind limb paresis, spades, uveitis, anisocoria, and urinary and stool incontinence. Blood tests were mostly uncommon, with the exception of mild hyperglobulinemia. The A / G ratio was 0.6. The cat was treated with 10 mg / kg GS-441524 SC SID for 3 weeks. Activity, mentation and uveitis improved within 72 hours of starting treatment. During the first 2 weeks, a slow improvement in mobility and eye symptoms was observed, but then a plateau was reached. After 3 weeks, the dose of GS-441524 was increased to 15 mg / kg GS-441524 SC SID due to persistent neurological and ocular deficits. In addition, enlargement of the left eye due to glaucoma was noted at this time and the eye continued to swell until it was removed at week 8 of treatment. Due to persistent weakness / lack of pelvic coordination and increasing lethargy, dose GS-441524 was increased to 20 mg / kg SC SID [or equivalent oral dose] at week 9 and 20 mg / kg SC BID was added to the regimen a few days later. GC376. Significantly increased activity and willingness to jump on elevated surfaces occurred within 48 hours of starting GS376 treatment. The combination treatment of GS-441524 and GC376 was maintained for 8 weeks. The cat has residual incontinence problems after treatment, but is otherwise clinically normal 6 months after treatment.
Boris - Maine Coon MI wet eye FIP
The five-month-old intact (uncastrated) Maine Coon cat, obtained from the breeder, had lethargy, anorexia, abdominal ascites, cough, anemia and neutrophilia. No biochemical analysis was performed to establish the diagnosis. The cat was treated with 6 mg / kg GS-441524 SC SID for 8 weeks. After six weeks of treatment, X-rays revealed nodules in the lungs, and after 8 weeks, hyperglobulinemia persisted. The GS-441524 dose was then increased to 8 mg / kg SC SID for 4 weeks. There was little improvement in blood tests and X-rays and the dose of GS-441524 was increased to 12 mg / kg SC SID over 4 weeks, followed by an increase to 17 mg / kg over 11 weeks, 25 mg / kg over 4 weeks and 30 mg / kg for 4 weeks. After 25 weeks of treatment, ultrasound revealed pleural abnormalities on the left side and X-rays showed no improvement in the pulmonary nodules. In addition, uveitis and retinal detachment have been reported in the right eye. Pulmonary aspirates that showed FIP-compliant inflammation were collected. After 33 weeks of treatment, 20 mg / kg SC BID GC376 was added to the regimen and the combined treatment of GS-441524 and GC376 was continued for 12 weeks. Increased activity was noted over several days. Over the course of 5 weeks, the weight gain accelerated, the cough subsided and the energy level increased. Blood tests showed an improvement in the A / G ratio, and chest X-rays showed a reduction in the lungs. After 84 days of combination antiviral therapy, the A / G ratio was 0.85 and the cat appeared clinically normal. The cat is currently 3 months after treatment.
References
Pedersen NC, Kim Y, Liu H, Galasiti Kankanamalage AC, Eckstrand C, Groutas WC, Bannasch M, Meadows JM, Chang KO. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J Feline Med Surg. 2018; 20 (4): 378-392.
Pedersen NC, Perron M, Bannasch M, Montgomery E, Murakami E, Liepnieks M, Liu H. efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. J Feline Med Surg. 2019; 21 (4): 271-281.
Perera KD, Rathnayake AD, Liu H, et al. Characterization of amino acid substitutions in feline coronavirus 3C-like protease from a cat with feline infectious peritonitis treated with a protease inhibitor. J. Vet Microbiol. 2019; 237: 108398. doi: 10.1016 / j.vetmic.2019.108398
Agostini ML, Andres EL, Sims AC, et al. Coronavirus susceptibility to the antiviral remdesivir (GS5734) is mediated by the viral polymerase and the proofreading exoribonuclease. MBio 2018; 9. DOI: 10.1128 / mBio.00221-18.
Pedersen NC. 2021. The neurological form of FIP and GS-441524 treatment. https://sockfip.org/the-neurological-form-of-fip-and-gs-441524-treatment/
Pedersen NC. The long history of beta-d-n4-hyroxycytidine and its modern application to treatment of covid019 in people and FIP in cats. https://sockfip.org/the-long-history-of-beta-d-n4-hydroxycytidineand-its-modern-application-to-treatment-of-covid-19-in-people-and-fip-in- cats /.
Agostini, ML et al. Small-molecule antiviral beta-dN (4) -hydroxycytidine inhibits a proofreading-intact coronavirus with a high genetic barrier to resistance. J. Virol. 2019; 93, e01348.
Warren, TK et al. Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 2016; 531, 381–385.
FIP Warriors CZ / SK - EIDD-2801 (Molnupiravir) https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/
Toots M, Yoon JJ, Cox RM, Hart M, Sticher ZM, Makhsous N, Plesker R, Barrena AH, Reddy PG, Mitchell DG, Shean RC, Bluemling GR, Kolykhalov AA, Greninger AL, Natchus MG, Painter GR, Plemper RK . Characterization of orally efficacious influenza drug with high resistance barrier in ferrets and human airway epithelia. Sci Transl Med. 2019; 11 (515): eaax5866.
Zdanowicz MM. The pharmacology of HIV drug resistance. Am J Pharm Educ. 2006; 70 (5): 100.doi: 10.5688 / aj7005100
Gandhi, S, Klein J, Robertson A, et al. De novo emergence of a remdesivir resistance mutation during treatment of persistent SARS-CoV-2 infection in an immunocompromised patient: A case report. medRxiv, 2021.11.08.21266069AID
Translator's note: The article contains information about the actual content of GS-441524 in tablets. However, this content may not correspond to the "equivalent" amount of GS-441524 in tablets from other manufacturers, where the actual content of GS-441524 is always slightly higher due to the known reduced bioavailability of the orally used drug. Therefore, it is not possible to simply and unambiguously compare the recommended dosage of GS-441524 from BOVA in Australia and here.
Introduction
Infectious feline peritonitis (FIP) is an infectious disease, especially of young cats. It occurs when a feline enteric coronavirus that multiplies in the gut undergoes a critical mutation that changes its tissue tropism from enterocytes to macrophages. The FIP virus then circulates in the body in macrophages - this is the ultimate mechanism of the Trojan horse. This leads to disseminated infection and the development of fibrinoid necrotizing vasculitis and serositis due to the deposition of immune complexes consisting of feline antibodies and FIP viral antigens.
In general, there are two forms of FIP - effusive ("wet") FIP and non-effusive ("dry") FIP. The disease process itself can occur in the abdomen, thoracic cavity, pericardium, eyes or central nervous system. Combinations of dry and wet FIP with various tissues are not uncommon.
Until recently, the diagnosis of feline infectious peritonitis (FIP) was a death judgment for a feline patient. In recent years, however, this vision has been turned upside down as a result of the pioneering work of Professor Niels C. Pedersen and colleagues at UC Davis.
Over the last 12 months, many veterinarians in Australia have also successfully managed many cases of FIP using remdesivir and GS-441524.
Omega-interferon (Virbagen) and polyprenyl immunostimulant (PPI) were the first drugs used to treat FIP, and both had some effects in some patients. Omega interferon has been useful in cases of effusive ("wet") FIP, often combined with low-dose prednisolone according to the Ishid protocol, while PPI, pioneered by Al Legendre, has been more useful in cases of non-fusible FIP. In some cases, both drugs were used at the same time. The problem was that both forms of therapy were often expensive, especially when both drugs were used, so that although patients improved and could have transient clinical remissions during treatment, permanent clinical cures were rare. As a result, most veterinarians still considered the diagnosis of FIP a prelude to euthanasia.
That all changed a few years ago thanks to the culmination of FIP's lifelong research. Niels Pedersen. Niels is an amazing North American veterinarian of Danish descent. He grew up on a chicken farm and originally wanted to be a clinician for large animals, but with great foresight he decided on a scientific career. Shortly after graduating, he traveled to Canberry to the John Curtin School of Medical Research at ANU, where in the late 1960s he received a PhD in kidney transplant rejection immunology from Professor Bede Morris, using sheep as an experimental model to study lymphocyte kinetics.
When Niels returned to UC Davis, he focused on studying infections and immunity. Although he has contributed to a large number of topics in internal medicine and the genomics of dogs and cats, FIP has become his favorite disease due to its commonness and current complexity. His studies date from the 1980s, when he specialized in diagnostics, virology and pathogenesis, to the present, with an increasing focus on therapy.
Niels, in collaboration with colleagues from Kansas State University, has shown that a purposefully designed protease inhibitor GC-376 could prevent and cure experimentally induced FIP in laboratory cats.1,2 Field clinical trials with cats with naturally occurring disease have been disappointing, especially when cats have had an ocular form of FIP or CNS disease. He did not give up, so he switched to another drug - GS-4415243,4 - a nucleoside analogue developed by the North American pharmaceutical company Gilead. This molecule has been shown to be much more effective than GC-376 in the treatment of FIP, both in experimental infections and in spontaneous cases of FIP. Starting with pharmacokinetics and dose escalation studies using a wide range of clinical cases, Niels and colleagues found that the required dose depended on whether the patient had dry or wet FIP and whether the eye or central nervous system (CNS) was affected.5
Surprisingly, Gilead, the manufacturer who developed GS441524, has not yet shown interest in developing this molecule for the treatment of cats. To fill the gap for effective FIP therapy around the world, various laboratories in China and Eastern Europe have begun producing GS-441524 and selling it on the black market.
The wide availability of the GS-441524, often of high quality and initially very high price, provided dedicated owners with a way to save their cats with FIP. Studies by clinical pathologist Samantha Evans of Ohio State University have indicated a cure rate of approximately 80 % in the field. Until recently, the procurement of the drug was complicated and full of problems, which at some level were circumvented by various "FIP Warriors" groups on Facebook. Unfortunately for Australian cat lovers, APVMA and Vet Boards finally understood what was going on and the Border Force made it much more difficult to obtain GS-441524 and its safe import for veterinary use. Regulatory and Veterinary Committees' warnings against prosecutors were directed against veterinarians who allowed cats with FIP to be treated with black market drugs.
Ironically, the COVID 19 pandemic provided a new solution to this problem. Gilead developed remdesivir (GS-5734) as a drug for the treatment of hepatitis C, Ebola and human coronavirus disease. Remdesivir is a prodrug of GS-441524, which contains an additional chemical side chain (including a phosphate group) to improve intracellular penetration (Figure 1B). Remdesivir (as a product of Veklura) obtained a temporary marketing authorization (for two years) from TGA in July 2020 for the treatment of SARS-CoV-2 infections in human patients with COVID-19. This registration process would normally take several years, but the severity of the pandemic has accelerated this process, taking into account preliminary data from clinical trials. As remdesivir became a licensed human drug and Gilead licensed production worldwide, it meant more access to quality raw material. This circumvented the problems with the use of the drug purchased on the black market, as well as the problems of unknown purity and consistency of the product over time.
In 2020, the veterinary compounding company BOVA Australia provided reliable supplies of remdesivir in a suitable format for IV and subcutaneous application. Studies in Australia have determined that the shelf life after reconstitution exceeds 12 days and have confirmed in vitro efficacy against coronaviruses in tissue cultures. The analytical purity of the drug is regularly checked by HPLC. Over the past year, veterinarians in every Australian state have used remdesivir to treat cats with FIP. There have been a number of effusive and non-fusive cases, including some cats with ocular disorders (uveitis) and others with multifocal CNS disease. Based on treatment of approximately 500 cats treated between October 2020 and November 2021, remdesivir has been shown to be highly effective in managing FIP infections. It allows for a slightly simpler subcutaneous administration and the injection appears to be slightly less painful compared to GS-441524 and does not cause the local injection site reactions observed with GS-441524 injection. Remdesivir was originally used exclusively in Australia, although it has also been available in the UK from BOVA UK for the last 2 months.
The molecular weight of remdesivir is 603 g / mol, while the molecular weight of GS-441524 is 291 g / mol. This could suggest that treatment of cats with remdesivir requires approximately twice the dose of GS-441524, although this does not take into account the possible improvement in intracellular penetration of remdesivir into certain tissues compared to GS-441524. The proposed dose of remdesivir in human patients with COVID19 is 200 mg intravenously (IV), followed by 100 mg IV daily. For a 70 kg human patient, this represents a daily dose of 1.3 mg / kg, so using allometric scaling, a dose of 5-10 mg / kg per day was considered correct for a cat. However, our experience with the first 500 cases was that many cats eventually needed a higher dose of remdesivir for permanent cure, so we adjusted our recommended dosage upwards (see below). Remdesivir provides BOVA as a sterile 10 mg / ml solution ready for use in a 10 ml vial.
Figure 1. (A) BOVA Remdesivir reconstituted and ready for treatment. After reconstitution, the contents of the vial are stable for at least 120 days at 5 ° C - and the vial is usually consumed in 3-7 days. It is best to store the vial in the refrigerator. (B) The pathway that remdesivir travels intracellularly to activate as GS-441524.
At present, Australia and the United Kingdom are the only countries where remdesivir is readily available by prescription for veterinary use. However, veterinarians in India, New Zealand, South Africa and parts of Europe have also started using human medicine suppliers to access the medicine.
Diagnosis
Figure 2: Amazingly comprehensive and practical overview of FIP diagnostics by Severine Tasker.
A complete differential diagnosis of FIP is beyond the scope of this article, but readers are strongly encouraged to read the excellent article by Séverine Tasker in the Journal of Feline Medicine & Surgery. 6
Although FIP can occur in cats of any age, most cases occur in kittens and cats less than 3 years of age. Persistent and often high fever that does not respond to antibiotic therapy (and often NSAIDs) is a common finding, as is increased plasma total protein levels due to elevated globulin concentrations (diffuse gammopathy in serum electrophoresis). In effusive or "wet" FIP, the albumin to globulin ratio may drop to <0.45. Acute phase reactants such as serum amyloid A and α1-acid glycoprotein tend to be markedly elevated. Many cats with FIP also exhibit secondary immune-mediated hemolytic anemia, increased AST and ALT activities, and jaundice.
Diagnostic imaging is crucial for early diagnosis, which has been greatly facilitated by the introduction of digital radiology and the widespread availability of diagnostic ultrasound in small animal practice. Pleural effusion is readily recognizable from chest X-rays, while abdominal effusion is best detected by ultrasound (Figure 3), especially if high frequency probes are available. It is worth noting that in some cases, the fluid pockets may be focal and localized. Often there is some fluid around the kidney under the kidney sheath, kittens may have scrotal edema, while in rare cases the discharge is limited to the pericardial sac. But the key is - to look for (i) effusion in any body cavity, (ii) granulomas in the kidneys, liver or lungs, (iii) enlarged intra-abdominal and mesenteric lymph nodes (Figure 5) or marked thickening of the iliac-ecological area (f focal FIP ’) ( Figure 5). Chest X-rays after drainage of pleural effusion may show changes corresponding to viral pneumonia.
Figure 2: (A) Ultrasound of the abdomen showing abundant highly echogenic fluid (fibrin fibers) in cats with high protein ascites due to effusive FIP. (B) The fusion contains a viscous yellow to straw-colored liquid. (C) An X-ray of the abdomen with the appearance of cut glass indicating fluid in the abdomen.
If you see an effusion - puncture - because fluid is the best diagnostic sample.
Figure 3: Marked mesenteric lymphadenomegaly in a cat with dry FIP.
A fluid with a high protein content, often yellow to straw in color, is characteristic (Figure 3B). If you see granuloma in the organ or if the lymph nodes are clearly enlarged - do FNA (thin needle aspiration biopsy), apply a smear, use RapidDiff staining and look for neutrophils and macrophages (pyogranulomatous inflammation) without visible infectious agents (Figure 4). The two diseases most commonly confused with FIP in adult cats are lymphoma and some types of lymphocytic cholangitis (associated with high protein ascites).
Figure 4: RapidDiff stained aspirate with a thin needle from the mesenteric lymph nodes of a 4-year-old oriental cat with dry FIP. Distinctive macrophages are the key to cytological diagnosis. Photo courtesy of Trish Martin.
Of course, effusive disease is much easier to diagnose because ascitic, pericardial or pleural fluid provides a suitable sample that can be examined cytologically, by fluid analysis and immunofluorescence (IFA) for FIP antigen, or reverse transcriptase PCR to detect FIP nucleic acid. IFA is performed at VPDS, B14, University of Sydney (via Vetnostics, QML, ASAP, VetPath, Gribbles or IDEXX). However, it is usually the cheapest way to send the sample directly to the university laboratory.
Dry FIP is more problematic because it usually requires a thin-needle aspiration biopsy of pyogranulomatous lesions in the liver, kidneys, or abdominal lymph nodes. Occasionally, cases of wet FIP may show fluid samples that are negative for IFA and / or PCR testing, but the patient is still likely to have FIP, which is reflected in a favorable response to remdesivir or GS-441524 treatment.
Treatment
Since October 2020, we have been treating cats with FIP with remdesivir (IV and SCI) and more recently with GS-441524 (oral), so our protocols are constantly evolving with experience. About 500 cats have been treated so far. We try to avoid being too prescriptive in our recommendations, as we suspect that there is no one-size-fits-all protocol and that each case presents unique circumstances, including patient size, whether the cat is still "happy" and reasonably , or is depressed and dehydrated. An important factor is the emotional and financial commitment of the owner. A key feature that needs to be mentioned is that both drugs are very safe, even in sick cats and kittens.
Note that the following recommended doses are higher than those originally recommended a year ago. Although lower doses worked in many patients, we found that this was often the wrong economic consideration, as disease recurrence at the end of treatment and the development of viral resistance during treatment appear to be related to insufficient initial dosing. So we have learned to be more aggressive from the beginning, which is cheaper in the long run (ie 2nd therapy is not required)
Our greatest experience is with remdesivir. This drug is expensive and the owner has to commit to a costly treatment process that takes 3 months. For most clients, this represents an emotional and financial burden. My view is that in many cases it is better to spend money on antiviral therapy as such than on extensive diagnostics and monitoring.
Figure 5: Significant thickening of the ilico-ecological area of the Devon Rex cat with the so-called "focal FIP", a common form of non-fusive FIP. Photo courtesy of Penny Tisdall.
One of the approaches in newly diagnosed cats with severe disease is hospitalization of cats during the first 3-4 days of treatment. Patients begin treatment with remdesivir when receiving IV fluid therapy (typically 2-4 ml / kg / hr; first day Hartmann's solution or Plasmalyte followed by 0.45 % NaCl and 2.5 % dextrose containing 20 mmol KCl / l). On the 1st day of hospitalization, remdesivir is administered in a high dose intravenously (10-15 mg / kg diluted in 10 ml with saline and is given SLOWLY for 20-30 minutes or longer, manually or by infusion pump; in human patients, administration lasts 2 hours. ) to achieve an increased starting dose of drug distribution volume. This achieves fast antiviral efficacy. In cases with CNS disease, we recommend a daily IV dose of 20 mg / kg. Many cats may appear slightly depressed several hours after IV remdesivir infusion. In human patients, remdesivir may cause infusion-related reactions, including low blood pressure, nausea, vomiting, sweating or chills, but we have not observed these events in our feline patients.
The advantage of starting treatment intravenously is that dehydration, if present, is corrected and you have IV access if you need to take other medicines (eg anticonvulsants, corticosteroids). Importantly, once an IV catheter is inserted, daily injections of remdesivir do not cause any pain or discomfort. However, if the cat eats and is diagnosed in the early stages of the disease, then IV therapy is not required and the same doses can be given subcutaneously, saving a lot of money.
FIP cats treated with remdesivir typically improve significantly during the first 2-3 days. However, we found that cases of effusion, and especially those that resulted in pleural effusion prior to treatment, should be closely monitored, as the combination of the antiviral effect of remdesivir and a higher than maintenance dose of crystalloids may lead to transient worsening of pleural effusion. This requires drainage twice a day using a 19G butterfly needle (1.1 mm - cream color) and a 3-way stopcock (ideally using an ultrasonic guide to find the best place to insert the needle). These "secondary" pleural effusions can be fatal if not detected in time and appear to occur in approximately 1 in 10 cases of effusive FIPs treated with remdesivir.
Another problem that occasionally occurs at this time is the development of neurological symptoms, including seizures. Our view is that this is not the effect of the drug as such, but rather the unmasking of the subclinical CNS FIP. Such cats require careful monitoring, while the development of seizures requires the use of anticonvulsant drugs such as midazolam (0.3 mg / kg IV), alfaxane or propofol (administered IV to be effective), followed by levetiracetam (Keppra) (10- 20 mg / kg, PO every 8 hours). Phenobarbitone is a reliable anticonvulsant, but it tends to increase the metabolism of many drugs, and levetiracetam is probably safer until we better understand the pharmacokinetics and metabolism of remdesivir and GS-441524. Some doctors also administer dexamethasone or prednisolone as a single treatment to relieve CNS inflammation.
Although advocating initial IV therapy for the most severe cases of FIP, cats and kittens that are still "happy" and eating do not require IV therapy at first and may instead begin subcutaneous injections at 10-12 mg / kg / day (20 mg / kg in CNS diseases). This is, of course, much cheaper because cats or kittens do not have to be placed in an infusion pump and hospitalized in a stressful environment. For clients who have financial limits, this may be a more appropriate way to start therapy. Some skilled colleagues, such as Jim Euclid, have developed a hybrid approach where kittens receive subcutaneous fluids daily as a bolus with injected remdesivir.
The cats were then given continuous subcutaneous injections of remdesivir. It originally took 84 days, and such cases accounted for most of the cases we have dealt with so far. Recently, we have been using aggressive IV / SCI remdesivir for initial therapy, and then cats are switching to oral GS-441524 for 10 weeks of consolidation therapy.
After the initial use of lower doses, which were not successful in every patient, we now use the following treatment protocols:
for cats with wet FIP: 10-12 mg / kg once daily (SID) for 2 weeks
for cats with severe eye impairment: 15 mg / kg SID by subcutaneous injection (SCI) for 2 weeks; Cats with severe uveitis should also be given topical corticosteroids (Before Forte or Maxidex) for 2-3 days (no longer!) and atropine eye ointment.
for cats with neurological FIP with CNS symptoms: administer 20 mg / kg SID SCI for 2-4 weeks. 5
It is important that owners are properly instructed on how to optimally administer daily injections. Cats will perceive the injection as less painful if the remdesivir solution in the syringe is allowed to warm to room temperature instead of being refrigerated. In addition, if you teach them simple tasks such as using a new needle when injecting (ie use a needle other than the one used to draw the medicine from the vial) and using 21G (0.8mm - green) or 23G diameter needles (0.6mm - blue), injections will be more tolerable. Although 21G needles are larger, some cats may have the advantage of injecting faster. Alternatively, for simplicity, veterinarians can prepare injections for the whole week, which they will keep in the refrigerator, and will give a new injection every day.
For cats that continue to perceive SC injections as painful, we used gabapentin orally (50 to 100 mg per cat) and / or transmucosally or SC administered buprenorphine 30-60 minutes before sedation / analgesia injection. The area to be injected can also be trimmed so that a topical EMLA cream can be applied 30 minutes before the injection. BOVA produces a faster-acting local anesthetic gel that may be useful in some patients. In exceptional cases, we inserted a cephalic catheter every 4-5 days so that owners could administer IV therapy instead of SC injections. Injection site reactions reported with GS-441524 injected abroad do not appear to occur with remdesivir.
After 2-4 weeks of taking remdesivir and after the abdominal fluid has disappeared and the ocular and CNS symptoms have improved or disappeared, we are now proposing a switch to GS-441524 tablets. This is done for 3 reasons: (i) it reduces costs (ii) eliminates the pain problem of SC injections (iii) in some patients it is more effective. Remdesivir injections are probably more reliable than oral GS-441524, and in the worst cases, you might choose to give them for 4 weeks, but for most cats, 2 weeks and comfort and lower oral formulation costs outperform everything else.
The use of GS-441524 tablets is relatively new in Australia but is widely used overseas. The recommended oral dose of GS441524 is generally the same as the SCI/IV dose of remdesivir: wet FIP cases receive 10-12 mg/kg PO SID, ocular cases 15 mg/kg PO SID and CNS cases 20 mg/kg (or higher). GS-441524 is more economical and is even safer than remdesivir. In CNS cases where large doses are given, it is probably best to give 10 mg/kg PO every 12 hours (BID) to circumvent the “ceiling” effect that has been reported in relation to limited absorption of high doses.
Figure 6. Focal dry FIP with pyogranulomatous inflammation of intra-abdominal lymph nodes. Instead of exploratory laparotomy, lymph node biopsy, histology, and immunohistology, 3 days of remdesivir IV treatment may be more cost-effective if FIP is highly suspected. Enlarged lymph node FNA is probably an ideal diagnostic option for physicians with this set of skills.
Why are the dosages about the same? At mg / kg, GS441524 has twice as many active molecules as remdesivir (due to the difference in their molecular weight), but the bioavailability of GS-441524 is only 50 % (only half of what is given is absorbed, and this is affected by feeding and also the effect of the ceiling dose) - so these two factors cancel each other out.
We recommend that GS-441524 tablets be given with a small treat to mask the tablet, with the main meal being served 1 hour later. The tablets provided by BOVA are 50 mg tuna-flavored tablets, with four score lines, so they can be divided into halves or even quarters.
In situations where owners cannot afford full treatment, we use mefloquine (Lariam; 5 mg / kg orally once daily in capsules or 62.5 mg twice a week) after initial treatment with remdesivir / GS-441524.
Phillip McDonagh, Jacqui Norris, Merran Govendir and colleagues at the Sydney School of Veterinary Science have shown that mefloquine has an antiviral effect. 7 This is probably due to the fact that mefloquine usurps the biochemical intracellular pathways used by the FIP virus, a mechanism that has recently been demonstrated with clofazimine. 8 (anti-leprosy medicine), and several other medicines. In several cats, where owners could not afford a complete treatment with remdesivir, mefloquine proved to be effective in reaching the limit of clinical cure.
The main advantage of buying remdesivir and GS-441524 from BOVA for the treatment of FIP cases is that the products we use are subject to quality control. It's just a prescription with the client's name and address, the patient's name and the dose to be given, and the compounder can usually deliver the vials or tablets to any veterinarian in Australia within 24-48 hours.
At present, the price is 100 mg of vials of remdesivir 250$ plus GST and postage (the total price is usually about 280$). GS-441524 is sold in packs of 10 tablets for 600$ plus shipping and handling. By purchasing more vials and tablets at the same time, of course, postage and handling fees will be reduced. We believe that most owners will feel much more comfortable getting a product from a well-known Australian company than sending money overseas and hoping that drugs of unknown quality on the black market will reach Australia safely without being detained by customs.
There is no reason why a well-motivated veterinarian would not be able to handle these cases in his own practice. This is often more convenient for the owner, especially if they struggle with daily injections and need a practice near them.
Figure 7: Gs-441524 tablets from BOVA Australia. They are tuna flavored. They can be divided into halves or even quarters. MUCH EASIER than injections for most cats. Less stress and less cost.
Veterinarians who wish to explore this option or have general questions about FIP case management may email Sally Coggins (dr.sallyc@gmail.com), Richard Malik (richard.malik@sydney.edu.au), David Hughes (concordvets@concordvets.com.au), Grette Howard (drgretta@gmail.com) or Professor Jacqui Norris (jacqui.norris@sydney.edu.au), for advice on diagnosis or treatment. Many Australian veterinarians interested in FIP have gained considerable expertise in the management of these cases. For example, Andrew Spanner in Adelaide treated more than 20 cases with excellent results. Thus, there are already many feline medicine physicians and internal medicine specialists with experience in the treatment of FIP, and so veterinarians who are hesitant to treat their own cases have the opportunity to recommend these specialists to their clients.
Physicians who accept FIP cases from GPs include: QLD Rhett Marshall, Marcus Gunew, Alison Jukes, Rachel Korman; NSW Katherine Briscoe, Michael Linton, Randolph Baral, Melissa Catt; VIC - Carolyn O'Brien, Keshuan Chow, Amy Lingard; WA-Martine Van Boeijen and Murdoch University Veterinary Hospital; TAS Moira van Dorsselaer.
All of these doctors (and probably even more we don't know about) are happy to accept cases for diagnosis and therapy. Everyone is probably happy to discuss case management with you.
Figure 8: Bengal kitten with CNS and ocular FIP (A: before) and (B: after) after Remdesivira. This cat also had pulmonary granulomas.
Sally Coggins, working with Lara Boland, Emily Pritchard, Associate Professor Mary Thompson and Professor Jacqui Norris at the Sydney School of Veterinary Science, is interested in treating cases with comprehensive diagnosis and free monitoring. It will be part of Sally's doctoral program, so you will help her advance in her studies by sending her cases. We hope that through these studies, we will get a better idea of how quickly cats respond and when exactly treatment can be safely stopped. Owners will only have to pay for remdesivir and GS-441524 for therapy. This group is also interested in treating cases with interferon-omega and mefloquine.
In most cases, FIP is doing very well with GS-441524 or remdesivir. Niels Pedersen has gathered an amazing resource for veterinarians interested in FIP case management - https://sockfip.org/dr - pedersen - research / . The site also provides some recommendations on how to monitor cats during treatment. I'm not very protocol-oriented, so the key things for me to keep track of are appetite, attitude, activity levels, and changes in body weight and fitness over time. Most physicians like to monitor serum hematology and biochemistry every month to ensure that all measurable abnormalities improve, although this can be stressful for the patient and increase treatment costs. The trade-off is taking a few drops of blood to monitor PCV, total plasma protein (TPP) using refractometry, and plasma color to determine if anemia is improving, jaundice is subsiding, and gamma globulin levels are lowering, resulting in lower TPP.
Do not worry about transient increases in globulin levels at the start of treatment; when high protein effusions are absorbed, a lot of immunoglobulins enter the patient's plasma. This phenomenon may be common until the 8th week of treatment, but disappears by the 12th week.
Figure 9: Transverse plane MRI image in contrast to T1 weighting. Note: dilatation of the lateral ventricles with very slight emphasis on the ependymal lining (orange arrows). Image courtesy of Christine Thomas.
And what about a kitten with multifocal CNS disease, where FIP CNS is the most likely cause of clinical symptoms? The traditional approach is serology (to rule out cryptococcosis and toxoplasmosis), a good history and thiamine test to rule out vitamin B1 deficiency, followed by MRI scans (Figure 9) and CSF collection for fluid analysis and multiplex neuro-qPCR analysis). This approach is very expensive and there is also a certain risk of anesthesia and especially CSF collection. We found that a 3-5 day intravenous or sc. Remdesivir therapy can be used as a therapeutic test in cats with probable CNS FIP and is a cost-effective alternative to complete diagnostic processing, which can cost 3-5000$ or more.
Similarly, if exploratory laparotomy, abnormal tissue biopsy, histology, and immunohistochemistry for FIP antigen are used to diagnose dry intra-abdominal FIP versus 3-5 days of treatment with remdesivir or GS-441524, a drug test may be considered, which is a better choice from in terms of patient well-being and reduced costs. Most cats with non-fusive FIP experience rapid improvement with antiviral therapy, with normalized fever, improved appetite, and better overall attitude within 2 to 3 days. If the patient does not respond to antiviral therapy, then exploratory laparotomy and representative organ biopsy are reasonable, as the main differential diagnoses are lymphoma and lymphocytic cholangitis.
This is a matter of personal approach for each doctor. FNA for cytological and sometimes immunohistochemical examination or PCR is a convincing non-invasive option where this expertise is available, but sometimes it does not give a definitive answer. Some veterinarians insist on tissue diagnosis and positive immunohistology or PCR in each patient, while others would like to "treat treatable" with a 3-5-day remdesivir / GS-441524 application and proceed to exploratory laparotomy only when there is no clear response to therapy.
It is incredibly satisfying to see the transformation of cats and kittens, which are not well, into normal and happy cats. It's really something that will lift your spirits as a doctor. It's good science and good veterinary medicine!
Conclusions
In the past, the diagnosis of FIP was an intellectual exercise so that we could end the suffering of a cat or kitten with the certainty of an accurate diagnosis. Now, thanks to FIP's lifelong study, Dr. Niels Pedersen, we are able to successfully treat perhaps 80 % or more cats with FIP if the client has sufficient funds. It is too early to predict whether or how many will be repeated later.
There is a need for intensive study in diagnosis and case management, but with the necessary effort, a good veterinarian should be able to work with a determined owner to achieve a clinical cure. The most important thing is not to put too many obstacles in the way of the dedicated owner and support him during the 12-week marathon treatment course by helping him find the best way to treat his patient. This may include sedative / analgesic treatment to help the cat improve controllability and prevent discomfort when the client brings their cat to the clinic daily for remdesivir injections or switching to GS-441524 tablets when the stress from the injections is too great for the owner. It is important to go a long way and a payment plan can be provided that will allow determined clients to improve the affordability of treatment.
Finally, the impact of COVID-19 on coronavirus research has been indeed profound, and several very promising drugs are under development, such as molnupiravir from Merck and another oral drug from Pfizer.
OVERALL SUMMARY
2-step approach to therapy
Phase 1 - INDUCTION
IV / SC injections of Remdesivir
For cats with wet FIP: 10-12 mg / kg remdesivir by subcutaneous injection (SCI) once daily (SID) for 2 weeks
For cats with eye: 15 mg / kg SID remdesivir SCI for 2 weeks
For cats with neurological symptoms of FIP and CNS: remdesivir 20 mg / kg SID for 2 weeks
Phase 2 - CONSOLIDATION
Switch to GS-441524 tablets after 2 weeks of remdesivir injection
For cats with wet FIP: 10-12 mg / kg GS-441524 oral SID for 10 weeks
For cats with eye impairment: 15 mg / kg SID GS-441524 oral SID for 10 weeks
For cats with neurological symptoms of FIP and CNS: GS-441524 10 mg / kg oral BID (20 mg / kg / day) for 10 weeks
References
Kim, Y .; Liu, H .; Galasiti Kankanamalage, AC; Weerasekara, S .; Hua, DH; Groutas, WC; Chang, KO; Pedersen, NC Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog. 2016, 12, e1005531.
Pedersen, NC; Kim, Y .; Liu, H .; Galasiti Kankanamalage, AC; Eckstrand, C .; Groutas, WC; Bannasch, M .; Meadows, JM; Chang, KO Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392.
Murphy, BG; Perron, M .; Murakami, E .; Bauer, K .; Park, Y .; Eckstrand, C .; Liepnieks, M .; Pedersen, NC The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies. Vet. Microbiol. 2018, 219, 226–233.
Pedersen, NC; Perron, M .; Bannasch, M .; Montgomery, E .; Murakami, E .; Liepnieks, M .; Liu, H. Efficacy, and safety of the nucleoside analog GS441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281.
Dickinson PJ, Bannasch M, Thomasy SM, et al. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. Journal of Veterinary Internal Medicine. 2020. doi: 10.1111 / jvim.15780.
Tasker S. Diagnosis of feline infectious peritonitis: Update on evidence supporting available tests. Journal of Feline Medicine and Surgery. 2018; 20 (3): 228-243. doi: 10.1177 / 1098612X18758592
McDonagh, P .; Sheehy, PA; Norris, JM Identification, and characterization of small molecule inhibitors of feline coronavirus replication. Vet. Microbiol. 2014, 174, 438–447.
Yuan, S., Yin, X., Meng, X. et al. Clofazimine broadly inhibits coronaviruses including SARS-CoV-2. Nature (2021). https://doi.org/10.1038/s41586-021-03431-4
https://sockfip.org/ - THE BEST resource on the internet or anywhere for FIP.
Figure 10: Two cats with dry FIP after successful therapy. As an avid young veterinarian wrote to me not so long ago - "that's why I did science!"
COSTS:
2 kg kitten with wet FIP 4 × 100 mg remdesivir vials - 1000$ 35 × 50 mg tablets GS-441524 - 2100$ Manipulation and GST - 30$ plus 310$ = 340$ A total of 3440$, approximately 290$ per week for 12 weeks
4 kg cat with dry FIP 7 × 100 mg remdesivir vials - 1750$ 70 × 50 mg tablets GS-441524 - 4200$ Handling and GST 30$ plus 600$ A total of 6550$, about 545$ per week for 12 weeks
Figure 11: Two siblings who developed FIP and were successfully treated with remdesivir and GS441524.
Beta-d-N4-hydroxycytidine is a small molecule (nucleoside) that was studied in the late 1970s in the former Soviet Union as part of biological weapons research [2]. The weaponization of diseases such as smallpox was a worldwide threat, but the danger of using the smallpox virus for this purpose was too great. Smallpox was eradicated from the world, virtually all stocks were destroyed and further research was banned. This led the US and the Soviet Union to research other RNA viruses as biological weapons and antivirals to defend against them. The Venezuelan equine encephalomyelitis virus (VEEV) was one of the first viruses to be seriously considered for use as a biological weapon. [3]. VEEV is transmitted to humans by mosquito bites and causes high fever, headaches and encephalitis with swelling that can be fatal. Beta-d-N4-hydroxycytidine has been found to inhibit not only VEEV replication but also a wide range of alphaviruses, including Ebola, chikungunya, influenza virus, norovirus, bovine diarrhea virus, hepatitis C virus and respiratory syncytial virus. [3-8]. The first reports of an inhibitory effect of beta-d-N4-hydroxycytidine on human coronavirus NL63 date back to 2006 [9]. Recent studies have confirmed its inhibitory effect on a wide range of human and animal coronaviruses [8].
An important part of the recent history of beta-d-N4-hydroxycytidine is associated with the Emory Institute for Drug Development (EIDD) [1], where he received the experimental designation EIDD-1931. The US government has provided significant financial support for the study of antivirals against alphaviruses in institutions such as Emory since 2004. [10]. In 2014, the Defense Threat Reduction Agency provided institutional support to find an antiviral compound against VEEV and other alpha-coronaviruses. "N4-Hydroxycytidine and its derivatives and antiviral uses" were included in U.S. Patent Application 2016/106050 A1 of 2016 [11]. Additional funding in 2019 was provided by the National Institute of Allergies and Infections for fellowship of the esterified beta-d-N4-hydroxycytidine precursor (EIDD-2801) for the treatment of influenza. [10]. The stated purpose of the chemical changes of EIDD-2801 was to increase its oral bioavailability, which would ultimately allow beta-d-N4-hydroxycytidine to be administered as pills and not as injections. In 2019/2020, the focus of research changed from influenza to SARS-CoV-2 [2]. The commercialization of EIDD-2801 was entrusted to Emory's Ridgeway Biotherapeutics subsidiary, which subsequently worked with Merck on a lengthy and costly FDA approval process. The current version of EIDD-2081 for field testing was named Molnupiravir.
Beta-d-N4-hydroxycytidine, the active substance in Molnupiravir, exists in two forms as tautomers. In one form, it acts as a cytidine with a single bond between the carbon and the N-OH group. In its other form, which mimics uridine, it has an oxime with a double bond between the carbon and the N-OH group. In the presence of beta-d-N4-hydroxycytidine, viral RNA-dependent RNA polymerase reads it as uridine instead of cytidine and inserts adenosine instead of guanosine. Switching between forms causes inconsistencies during transcription, which results in numerous mutations in the viral genome and a cessation of viral replication. [8].
Merck's commitment to conditional and full FDA approval of Molnuparivir continues. In its statement, Merck stated: [12]"In anticipation of the results of the MOVe-OUT program, Merck manufactures Molnupiravir at its own risk. Merck expects to produce 10 million therapeutic doses by the end of 2021, with more expected to be produced in 2022. Merck is committed to providing timely access to Molnupiravir worldwide, if authorized or approved, and plans to introduce access to tiered prices based on World Bank admission criteria that reflect countries' relative ability to fund their pandemic health response. As part of its commitment to extend the global approach, Merck has previously announced that it has entered into non-exclusive voluntary licensing agreements for Molnupiravir with established generic manufacturers to accelerate the availability of Molnupiravir in more than 100 low and middle income countries (LMICs) following approval or emergency approval by local regulatory agencies. . " This "generosity" is unlikely to apply to use in animals.
Drugs to inhibit the current Covid-19 pandemic have been the subject of accelerated field trials in the last two years, and one of them, Remdesivir, has been approved for use in hospitalized patients in record time. Last year, Molnupiravir was submitted for conditional approval as an oral medicinal product for home treatment of the infection at an early stage. [12]. However, anti-coronavirus compounds have been developed previously for another common and serious feline disease, feline infectious peritonitis (FIP). These drugs include a protease inhibitor (GC376) [13] and an RNA-dependent RNA polymerase inhibitor (GS-441524), which is an active ingredient of Remdesivir [14]. The success of antiviral drugs in the treatment of FIP prompted a recent study by EIDD-1931 and EIDD-2801 for their ability to inhibit FIPV in tissue cultures. [15]. The effective EC50 concentrations for EIDD-1931 against FIPV are 0.09 μM, EIDD-2801 0.4 μM and GS441524 0.66 μM [15]. The percentage of cytotoxicity at 100 μM is 2.8, 3.8 and 0, respectively. Therefore, EIDD-1931 and EIDD-2801 are slightly more effective at inhibiting viruses, but also more cytotoxic than GS-441524. These laboratory studies suggest that EIDD-1931 and EIDD-2801 are excellent candidates for the treatment of FIP.
Although EIDD-1931 and EIDD-2801 are a great promise for the treatment of FIP, there are several obstacles that will make the legal use of these compounds unlikely in the near future. GS-441524, the active form of Remdesivir and patented by Gilead Sciences, was investigated for use in cats with FIP shortly before the Covid-19 pandemic. FIP research [14] therefore stimulated the potential use of Remdesivir against Ebola and not SARS-like coronavirus [14]. Although these studies were conducted in collaboration with scientists from Gilead Sciences, the company refused to grant GS-441524 rights to treatment in animals as soon as it became clear that there was a much larger market for Covid-19 in humans. [16]. Similarly, my attempts over the past 2-3 years at Emory, Ridgeback Biotherapeutics, and Merck Veterinary Division to investigate EIDD-1931 and EIDD2801 for the treatment of FIP in cats have either remained unanswered or rejected, no doubt for similar reasons why Gilead refused to grant rights for GS-441524. However, the great worldwide need for FIP treatment quickly supported the unapproved market for GS-441524 from China. The same need to treat FIP has recently aroused interest in Molnupiravir, also from China.
Situation with EIDD-1931 vs. EIDD-2801 / Molnupiravir and GS-441524 vs. Remdesivir raises the question of why some medicines are being converted to prodrugs for marketing purposes [17]. Remdesivir was reportedly esterified to increase antiviral activity, although studies in cats showed that GS-441524 and Remdesivir had similar viral inhibitory activity in tissue culture. [18]. However, Remdesivir was found to be poorly absorbed by the oral route and was therefore conditionally approved for injectable use only. EIDD-2801 was designed to increase the oral absorption of EIDD-1931, although previous research has shown that EIDD-1931 is well absorbed orally without esterification. [6]. The motives for the commercialization of Remdesivir instead of GS-441524 for human use have been scientifically questioned, as it appears to be better in several ways without further modification. [17]. Why EIDD-2801 was chosen for commercialization, when EIDD-1931 would be cheaper, 4 times more effective against viruses and one third less toxic than EIDD-2801 [15]? The strength of patent rights and the longevity of patents may be more important factors in these decisions. [16,17,19].
One of the problems in the treatment of FIP in cats is the blood-eye and blood-brain barriers, which become very important when the disease affects the eyes and / or the brain. [13, 14, 20]. This problem has been largely overcome in the treatment of ocular and neurological forms of FIP with GS-441524 by gradually increasing the dose to increase blood levels and thus drug concentrations in the ventricular fluid and / or brain. [20]. GC376, one of the most effective antivirals against FIP virus in culture [17], is not effective against ocular and neurological FIP due to the inability to get enough drug to these sites, even if the dose is increased several times[14]. Fortunately, it appears that EIDD-1931 can reach effective levels in the brain, as indicated by studies in horses with VEEV infection. [3]. Drug resistance is another problem that now occurs in some cats treated with GS-441524, especially in individuals with the neurological form of FIP. Long treatment procedures and difficulties in transporting enough drug to the brain support the development of drug resistance.
The short-term and long-term toxic effects of the drug candidate on the test person or animal are crucial. GS-441524 showed lower toxicity in cell cultures than GC376, EIDD-1931 and EIDD-2801 [15]. Most important, however, is the toxicity that manifests itself in vivo. GC376 is one of the drugs with the highest coronavirus inhibitory effect [15], but slows the development of adult teeth when given to young kittens [13]. No serious toxicity was observed during nearly three years of field use of GS-441524, reflecting the complete absence of cytotoxic effects in vitro at concentrations up to 400 µM. [18]. However, EIDD-1931 and EIDD-2801 show significant cytotoxicity at 100 μM [15]. Therefore, the ability of EIDD-1931 to make fatal mutations in RNA has been raising a number of questions for some time. [8, 21, 22]. This was the main reason why the application for the treatment of diseases was still delayed. However, the current recommended duration of treatment with Covid-19 Molnupiravir is only 5 days at the initial stage of treatment. [10]. However, the recommended duration of FIP treatment with GS-441524 is 12 weeks [14], which represents a much longer time for the manifestation of toxicity. Therefore, close observation of cats during treatment with EIDD-1931 or EIDD-2801, whether short-term or long-term, will be important.
All existing antiviral drugs have led to the development of drug resistance through mutations in the viral genome. Although Remdesivir appears to be less susceptible to such mutations compared to drugs used in viral diseases such as HIV / AIDS, resistance is well documented. [23-25]. Resistance to GS-441524 in cats treated for FIP was observed at a higher frequency, especially in cats with neurological FIP, where it is more difficult to deliver sufficient drug to the brain [13, 14, 20]. Resistance to GS-441524 in cats is also likely to be a major problem, as cats with FIP are often treated for 12 weeks or longer, while Remdesivir (and Molnupiravir) are recommended for only five days during the initial viremic stage of Covid-19. [16]. The problem of drug resistance in HIV / AIDS treatment is effectively addressed by using a cocktail of different drugs simultaneously with different resistance profiles. Mutants resistant to one drug will immediately inhibit other drugs, thus preventing their positive selection during treatment. Inhibition of resistance is particularly strong when the two drugs attack different proteins involved in virus replication. For example, GC376 is a protease inhibitor [13], while GS-441524 acts on an RNA-dependent RNA polymerase [18]. However, GC376 is not as well absorbed across the blood-brain barrier. Although the necessary research has not yet been performed, there appears to be no cross-resistance between GS-441524 and Molnupiravir and is as effective as GS-441524 in crossing the blood-brain barrier. [3]. This makes Molnupiravir (or 5-hydroxycytidine) an important contribution to the future treatment of FIP.
As expected, Molnupiravir has recently been tested on cats with FIP by at least one Chinese retailer, GS-441524, and preliminary results are available on the FIP Warriors website. [26]. Field trials included 286 cats with various forms of naturally occurring FIP observed at pet clinics in the United States, the United Kingdom, Italy, Germany, France, Japan, Romania, Turkey, and China. The 286 cats that participated in the study, including seven cats with ocular (n = 2) and neurological (n = 5) FIP, did not die. Twenty-eight of these cats were cured after 4-6 weeks of treatment and 258 after 8 weeks. All treated cats were healthy after 3-5 months, a period during which relapses would be expected to relapse unsuccessfully. These data provide convincing evidence of the safety and efficacy of Molnupiravir in cats with various forms of FIP. However, we hope that this field study will be written in manuscript form, submitted for review and published. Either way, Molnupiravir is already marketed to owners of cats with FIP. At least one other major retailer of GS-441524 is also interested in using Molnupiravir for FIP, indicating a demand for additional antiviral drugs for cats with FIP.
Safe and effective dosing for Molnupiravir in cats with FIP has not been published. However, at least one vendor from China provided certain pharmacokinetic and field test data for Molnuparivir in cats with naturally occurring FIP in a leaflet for the product Hero-2081. [26]. However, this information does not clearly indicate the amount of Molnupiravir in one of their "50 mg tablets" and the actual dosing interval (q12h or q24h?). Fortunately, the estimated starting dose of molnupiravir for cats with FIP can be obtained from published in vitro cell culture studies of EIDD-1931 and EIDD-2801. [15] and laboratory and field studies GS-441524 [14,18]. Molnupiravir (EIDD-2801) has an EC50 of 0.4 μM / μl against FIPV in cell culture, while the EC50 of GS-441524 is about 1.0 μM / μl. [18]. Both have a similar oral absorption of about 40-50 %, so the effective subcutaneous (SC) dose for Molnupiravir would be approximately half the recommended 4 mg / kg SC every 24 hours of the initial dose for GS441524. [14] or 2 mg / kg SC q24h. The per-os (PO) dose would be doubled to account for less effective oral absorption at a dose of 4 mg / kg PO every 24 hours. The estimated initial oral dose of molnupiravir for cats with FIP can also be calculated from the available Covid-19 treatment data. Patients treated for Covid-19 are given 200 mg of molnupiravir PO q12h for 5 days. This dose was evidently calculated from a pharmacokinetic study performed in humans, and if the average person weighs 60-80 kg (70 kg), the effective inhibitory dose is 3,03.0 mg / kg PO q12h. The cat has a basal metabolic ratio 1.5 times higher than humans, and assuming the same oral absorption in both humans and cats, the minimum dose for cats according to this calculation would be 4.5 mg / kg PO every 12 hours. Assuming that molnupiravir crosses the blood-brain barrier and the blood-brain barrier as efficiently as GS-441524 [3,18], the dose would be increased ~ 1.5 and ~ 2.0-fold to allow adequate penetration into the aqueous humor and cerebrospinal fluid for cats with ocular (~ 8 mg / kg PO, q12 h) or neurological FIP (~ 10 mg / kg PO, q12h). The treatment will last 10-12 weeks and the monitoring of the response to treatment will be identical to GS-441524 [14, 20]. These recommendations are based on published data assumptions and further experience with Molnupiravir will be required in this area. Molnupiravir is unlikely to be safer and more effective than GS-441524 in the treatment of FIP, but a third antiviral drug may be particularly useful in preventing resistance to GS-441524 (as a cocktail of antivirals with different resistance profiles) or in treating cats that no longer respond. good on GS-441524. It is largely unknown whether Molnupiravir will be without long-term toxic effects, as the active substance N4-hydroxycytidine is an extremely potent mutagen. [21] and the duration of FIP treatment is much longer than with Covid-19 and there is a likelihood of major side effects.
It is a pity that EIDD-1931 (N4-hydroxycytidine), the active substance in Molnupiravir, has not received much attention in the treatment of FIP cats than Molnupiravir. EIDD-1931 has a 4-fold greater inhibitory effect against the virus than Molnupiravir (EC50 0.09 vs. 0.4 μM) and the percentage of cytotoxicity is slightly lower (2.3% vs. 3.8% at 100 μM) [15]. N4-hydroxycytidine is also efficiently absorbed orally [3], which was downplayed in the development of EIDD-2801 (Molnupiravir). This scenario is identical to the GS-441524 vs. Remdesivir, the second of which, Remdesivir, was chosen for commercialization, although current research suggests that GS-441524 would be the best candidate.[17].
References
Painter GR, Natchus MG, Cohen O, Holman W, Painter WP. Developing a direct acting, orally available antiviral agent in a pandemic: the evolution of molnupiravir as a potential treatment for COVID-19 [published online ahead of print, 2021 Jun 18]. Curr Opin Virol. 2021; 50: 17-22. doi: 10.1016 / j.coviro.2021.06.003
Halford B. An emerging antiviral takes aim at COVID-19. c & en topics. 2020. https://cen.acs.org/pharmaceuticals/drug-development/emerging-antiviral-takes-aim-COVID19/98/web/2020/05.
Painter GR, Richard A. Bowend RA, Bluemling GR et al. The prophylactic and therapeutic activity of a broadly active ribonucleoside analog in a murine model of intranasal Venezuelan equine encephalitis virus infection. Antiviral Res. 2019, 171: 104597
Costantini, VP, Whitaker, T., Barclay, L., Lee, D., McBrayer, TR, Schinazi, RF, Vinje, J., 2012. Antiviral activity of nucleoside analogues against norovirus. Antivir. Ther.17 (6), 981–991. https://doi.org/10.3851/imp2229.
Ehteshami, M., Tao, S., Zandi, K., Hsiao, HM, Jiang, Y., Hammond, E., Amblard, F., Russell, OO, Merits, A., Schinazi, RF, 2017. Characterization of beta-dN (4) -hydroxycytidine as a novel inhibitor of chikungunya virus. Antimicrob. Agents Chemother. 61 (4) e02395-02316. https://doi.org/10.1128/aac.02395-16.
Stuyver, LJ, Whitaker, T., McBrayer, TR, Hernandez-Santiago, BI, Lostia, S., Tharnish, PM, Ramesh, M., Chu, CK, Jordan, R., Shi, J., Rachakonda, S ., Watanabe, KA, Otto, MJ, Schinazi, RF, 2003. Ribonucleoside analogue that blocks replication of bovine viral diarrhea and hepatitis C viruses in culture. Antimicrob. Agents Chemother. 47 (1), 244–254.
Yoon J., Toots M, Lee S, Lee ME, et al., 2018. Orally efficacious broad-spectrum ribonucleoside analog inhibitor of influenza and respiratory syncytial viruses. Antimicrob. Agents Chemother. 2018, 62 (8): https://doi.org/10.1128/aac.00766-18
Urakova N, Kuznetsova V, Crossman DK, Sokratian A, Guthrie DB, Kolykhalov AA, et al. β-d-N4Hydroxycytidine is a potent anti-alphavirus compound that induces a high level of mutations in the viral genome. J Virol. 2018, 92: e01965 – e01917. doi: 10.1128 / JVI.01965-17.
Pyrc, K., Bosch, BJ, Berkhout, B., Jebbink, MF, Dijkman, R., Rottier, P., van der Hoek, L., 2006. Inhibition of human coronavirus NL63 infection at early stages of the replication cycle . Antimicrob. Agents Chemother. 2006, 50 (6): 2000–2008. https://doi.org/10.1128/aac.01598-05.
Whitfill T. A likely new treatment for Covid-19 was made possible by government-funded innovation. STAT +. https://www.statnews.com/2021/10/05/government-funding-backed-molnupiravir-possible-newcovid-19-treatment/.
Painter, GR, Guthrie, DB, Bluemling, G., Natchus, MG N4-Hydroxycytidine and Derivatives and Antiviral Uses Related Thereto. US Patent Application, 2016, 2016/106050 A1.
Merck news release, October 1, 2021. https://www.merck.com/news/merck-and-ridgebacksinvestigational-oral-antiviral-molnupiravir-reduced-the-risk-of-hospitalization-or-death-by-approximately -50percent-compared-to-placebo-for-patients-with-mild-or-moderate /.
Pedersen NC, Kim Y, Liu H, Galasiti Kankanamalage AC, Eckstrand C, Groutas WC, Bannasch M, Meadows JM, Chang KO. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J Feline Med Surg. 2018, 20 (4): 378-392.
Pedersen NC, Perron M, Bannasch M, Montgomery E, Murakami E, Liepnieks M, Liu H. efficacy and safety of the nucleoside analog GS-441524 for the treatment of cats with naturally occurring feline infectious peritonitis. J Feline Med Surg. 2019, 21 (4): 271-281.
Cook SE, Vogel H and D. Castillo D. A rational approach to identifying effective combined anticoronaviral therapies against feline coronavirus. 2021. bioRxiv 2020.07.09.195016; doi: https://doi.org/10.1101/2020.07.09.195016
Zhang S. A Much-Hyped COVID-19 Drug Is Almost Identical to a Black-Market Cat Cure. May 8, 2020 Shutterstock / The Atlantic, https://www.theatlantic.com/science/archive/2020/05/remdesivir-cats/611341/.
Yan VC, Muller FL. Advantages of the Parent Nucleoside GS-441524 over Remdesivir for Covid-19 Treatment. ACS Medicinal Chemistry Letters. 2020, 11 (7): 1361-1366 DOI: 10.1021 / acsmedchemlett.0c00316
Murphy BG, Perron M, Murakami E, Bauer K, Park Y, Eckstrand C, Liepnieks M, Pedersen NC. The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies.Vet Microbiol. 2018, 219: 226-233.
Common Dreams. Public citizen. Press release, August 4, 2020, https://www.commondreams.org/newswire/2020/08/04/public-citizen-scientists-gilead-and-federalscientists-have-neglected
Dickinson PJ. Coronavirus Infection of the Central Nervous System: Animal Models in the Time of Covid-Front. Vet. Sci. 2020, 23: https://doi.org/10.3389/fvets.2020.584673
Zhou S, Hill CS, Sarkar S, et al., Β-d-N4-hydroxycytidine Inhibits SARS-CoV-2 through lethal mutagenesis but Is also mutagenic to mammalian cells. J Infect Dis. 2021, 224: 415–419, https://doi.org/10.1093/infdis/jiab247.
Cohen J, Piller C. Emails offer look into whistleblower charges of cronyism behind potential COVID-19 drug. ScienceInsider-Health. 2020, https://www.science.org/news/2020/05/emails-offer-look-whistleblowercharges-cronyism-behind-potential-covid-19-drug.
Agostini ML, Andres EL, Sims AC, et al. Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease. MBio 2018; 9. DOI: 10.1128 / mBio.00221-18.
Szemiel AM, Merits A, Orton RJ, In vitro selection of Remdesivir resistance suggests evolutionary predictability of SARS-CoV-2. Plos Path, 2021, https: //doi.org/10.1371/journal.ppat.1009929.
Martinot M, Jary A, Fafi-Kremer S, et al., Emerging RNA-Dependent RNA Polymerase Mutation in a Remdesivir-Treated B-cell Immunodeficient Patient With Protracted Coronavirus Disease 2019, Clinical Infectious Diseases, 2020 ;, ciaa1474, https: / /doi.org/10.1093/cid/ciaa1474
FIP Warriors CZ / SK - EIDD-2801 (Molnupiravir) https://www.fipwarriors.eu/en/eidd-2801-molnupiravir/
Original article: SUMMARY OF GS-441524 TREATMENT FOR FIP Niels C. Pedersen, DVM PhD, Professor Emeritus, Pet Health Center, School of Veterinary Medicine, UC Davis
We use the same criteria to monitor treatment as described in clinical study published in JFMS (Journal of Feline Medicine and Surgery). Owners should monitor temperature, weight, activity, appetite, and clinical signs of the original disease at daily or weekly intervals. Blood tests - hematology and biochemistry (including serum protein values - total protein, albumin, globulin, A: G ratio) at the beginning of treatment and then every 4 weeks. It is always useful to update these values along with the weight in the form of a graph. The aim is to have a healthy, sensitive and active cat at the end of 12 weeks of treatment and with normal blood test values, especially in terms of hematocrit, total protein, globulin, albumin and A: G ratios. Significant weight gain is also a good sign, and some young or particularly emaciated cats can more than double their weight during treatment. This is, of course, an idealized treatment, and it should be appreciated that upward adjustments may be required if the response is slow or if complications such as ocular or neurological impairment occur during treatment.
Supportive (symptomatic) care may be required to stabilize cats that are critically ill at the time of diagnosis or during the first days of treatment with GS-441524 (GS). Abdominal effusion should not be aspirated unless it compresses the chest and interferes with respiration, as it is quickly replaced at the expense of the rest of the body. However, thoracic effusions are usually associated with varying degrees of dyspnoea and should be eliminated. Chest effusions return much more slowly. Symptomatic care also often includes fluids and electrolytes to suppress dehydration, antibiotics suspected of secondary bacterial infection and anti-inflammatory drugs (usually systemic corticosteroids), and rarely blood transfusions. Some cats with eye problems may also need topical medications to suppress severe inflammation and increased intraocular pressure (glaucoma).
Corticosteroids such as prednisolone should only be used during the first days of GS treatment and should be discontinued when there is a rapid improvement in health. Long-term use of corticosteroids with GS is strongly discouraged as it may mask the signs of improvement caused by GS, especially in cats with neurological FIP, has no therapeutic power and may interfere with the development of a protective immune response to FIP. It is possible that this immune response plays a major role in the final cure. If cats are on chronic steroid therapy, no dose reduction is required as there is no evidence that cats experience severe adrenal atrophy, which occurs in humans during long-term steroid therapy. Many owners, GS treatment consultants and veterinarians will use various promoted supplements to improve liver, kidney or immune system health, as well as vitamins such as B12. These substances do not have proven effectiveness and I consider them a waste of money.
Treatment with GS, which is the most common, can also be complicated by ulcers / lesions at the injection site. Treatment is difficult for both owners and cats because injections can be painful. In some cats, especially those with neurological impairments, there is a problem with the development of partial drug resistance, which requires an increase in dose. The response to treatment is usually within 24-72 hours and most cats return to normal or approach normal within 2-4 weeks, which is a good sign. We anticipate that the success rate of FIP treatment with GS-441424 is greater than 80%, given treatment failure due to misdiagnosis of FIP, inappropriate dosing, health complications, and drug resistance. Young cats are easier to treat and have a higher cure rate than cats older than 7 years. Cats with wet or dry FIP, with uncomplicated neurological or ocular symptoms, are easier to treat than cats with neurological FIP.
The starting dose for cats with wet or dry FIP without signs of ocular or neurological disease is 4-6 mg / kg daily for 12 weeks, with younger cats and wet FIP tending toward the lower limit and dry cases to the upper limit. Cats with ocular lesions and no neurological symptoms start with a dose of 8 mg / kg daily for 12 weeks. Cats with neurological symptoms start at a daily dose of 10 mg / kg for 12 weeks. If cats with wet or dry FIP initially show ocular or neurological symptoms, they switch to appropriate ocular or neurological doses. There is an oral form of GS available from at least two sources in China (Spark, Mutian), but I do not use it, so I do not know a comparable dosage. However, I do not recommend this if the injection dose rises above 10 mg / kg per day, as the effectiveness of oral absorption decreases at these high doses.
I recommend adjusting the dosage by weekly weight control. The weight gain of many of these cats can be huge, either because they are so skinny at first or they grow, or both. If weight loss occurs at the beginning of treatment, I remain at the original dose and do not reduce it. Failure to gain weight during treatment is considered a bad sign. We do not increase the dose unless there are serious reasons for this, such as worsening or improved blood test results, slow improvement, poor activity, restoration of the original clinical symptoms, or a change in the form of the disease, including ocular or neurological symptoms. This is where common sense comes in, because you don't want to get stuck on one blood level, which is not quite common, but does not affect the overall health of the cat. For example, globulin may still be a little high, but other important blood test values and health are very good. If there is a good reason to increase the dose, it should always be from +2 to +5 mg / kg per day and for at least 4 weeks. If these 4 weeks cause a prolongation of the 12-week duration of treatment, it is because of this dose adjustment. A positive response to any dose increase can be expected, and if you do not see an improvement, it means that the dose is still not high enough, drug resistance is developing, you have a bad GS brand, the cat does not have FIP, or there are other diseases that affect treatment.
One of the most difficult decisions is determining when to stop treatment. Although some cats, often younger with wet FIP, can be cured as early as 8 weeks, and possibly earlier, the usual duration of treatment is 12 weeks. Some cats may even require a dose adjustment and longer treatment periods. Critical blood levels such as hematocrit, total protein, albumin and globulin levels, and total white blood cell and absolute lymphocyte counts usually return to normal in treated cats after 8-10 weeks, when there is often an unexpected increase in activity levels. It is assumed, but there is no evidence yet, that after 8-10 weeks, the cat will develop its own immunity to infection. This is a situation that occurs in the treatment of hepatitis C in humans, which is also a chronic infection caused by the RNA virus, which often requires up to 12 or more weeks of antiviral treatment.
Unfortunately, there is no simple test to determine when a cure has taken place, and the fear of relapse often leads owners, treatment advisers and veterinarians to extend treatment beyond 84 days. Fear of relapses will also make people involved in the decision-making process too cautious about a single blood value that is slightly abnormal (eg, slightly high globulin or slightly low A: G ratio), or final ultrasound results suggesting suspected enlarged lymphatics. nodules, small amounts of fluid in the abdomen, or vague irregularities in organs such as the kidneys, spleen, pancreas, or intestines. It should be borne in mind that although most animals fall within the normal range of blood values, they are otherwise bell-shaped curves, and that there are a few exceptional patients who will have values at the edge of these curves. The ultrasound diagnosis must take into account the degree of pathology that may occur in the abdominal cavity affected by FIP, such as scars or some consequences in the form of organ changes in successfully treated cats. In situations where such questions arise, it is better to look more closely at the overall picture, and not just at one small part. The most important outcome of treatment is a return to normal health, which has two components - external health symptoms and internal health symptoms. External signs of health include a return to normal activity levels, an appetite, adequate weight gain or growth, and coat quality. The latter are often one of the best measures of health for a cat. Internal health symptoms are manifested by the return of certain critical values to normal based on periodic monitoring of complete blood counts and biochemistry. The most important values in the blood count are the hematocrit and the relative and absolute total number of white blood cells, neutrophils and lymphocytes. The most important values in biochemistry (or serum electrophoresis) are total protein, globulin, albumin and A: G ratio. Bilirubin is often elevated in cats by effusive FIP and may be useful in monitoring the severity and duration of inflammation. There are many other values in hematology and biochemistry panels, and it is not uncommon for some of them to be slightly higher or lower than normal, and it is better to ignore these values unless they are significantly elevated and associated with clinical symptoms - such as high urea and creatinine, which are also associated with increased water consumption, excessive urination, and abnormalities in urine analysis. The number of platelets in cats is notoriously low due to the trauma of blood collection and platelet aggregation, and should always be verified by a manual blood smear test. The final decision to discontinue or extend treatment when you encounter unclear doubts about different test procedures should always be based on external health manifestations more than on any single test result.
Different FIP groups have come up with different modifications of FIP treatment. Some groups will treat with an extremely high dose of GS from the beginning instead of increasing the dose only when indicated, or increase their GS dose in the last two weeks, or postpone treatment with a higher dose of GS in the hope of shortening the next two weeks. duration of treatment or reduce the likelihood of relapse. Some advocate the use of interferon omega or non-specific immunostimulants to further stimulate the immune system, and some use various other modifications. There is no evidence that modification of the extra high dose treatment will improve the cure rate. Similarly, interferon omega and non-specific immunostimulants have no demonstrated beneficial effects in FIP when administered as a single treatment or as adjuncts to GS. The practice of adding another antiviral drug, the viral protease inhibitor GC376, to the treatment of GS in cats that develop resistance to GS is also emerging, but this possibility still requires research. Finally, it is common for owners, treatment groups and veterinarians to add many supplements, tonics or injections (eg B12) to increase blood levels or to prevent liver or kidney disease. Such supplements are rarely needed in cats with pure FIP.
FIP relapses during the 12-week post-treatment observation period occur, and there is no simple blood test to predict whether a cure has occurred or is possible. Relapses usually involve infections that have entered the central nervous system (brain, spine, eyes) during treatment with wet or dry FIP, which has not been accompanied by neurological or ocular symptoms. The dose of GS-441524 used to treat these forms of FIP is often insufficient to effectively overcome the blood-brain or blood-eye barrier. The blood-brain barrier is more inaccessible than the blood-eye barrier, which explains why eye lesions are easier to treat than brain or spinal infections. Relapses that occur in the post-treatment period and that involve the eyes, brain or spine are usually treated for at least 8 weeks at an initial daily dose at least 5 mg / kg higher than the dose used during the primary treatment (eg 10, 12, 15 mg / kg daily). It is recommended that GS oral formulations not be used if the dose exceeds 10 mg / kg daily for injection, as intestinal absorption efficiency is reduced at high oral concentrations. Cats that cannot be cured of the infection at doses up to 15 mg / kg per day are likely to develop varying degrees of resistance to GS-441524. Partial resistance may allow the symptoms of the disease to be kept under control but not cured, while general resistance manifests itself in varying severity of clinical symptoms during treatment.
At the time of diagnosis, there may be resistance to GS-441524, but this is unusual. Rather, it occurs during treatment, and is often partial at first, leading to the need for higher dosing. In some cats, it may become complete. Resistance is a major problem in cats with neurological disease, especially those that have neurological symptoms or develop a brain infection during treatment, or during relapse after treatment has appeared to be successful. Many cats with partial drug resistance can be treated for signs of the disease, but relapse occurs as soon as treatment is stopped. The cats have been "treated" at the FIP for more than a year without healing, but eventually the resistance worsens or the owner runs out of money.
GS-441524 treatment shows no or minimal systemic side effects. It may cause mild kidney damage in some cats, but should not lead to kidney failure. Systemic vasculitis-type drug reactions have been observed in several cats and can be confused with injection site reactions. However, these drug reactions are in non-injectable areas and often go away on their own or respond well to short-term low-dose steroids. The main side effect of GS treatment is pain at the injection sites, which varies from cat to cat and according to the abilities of the person giving the injections (usually the owner). Injection site ulcers / lesions are a problem in some cats and usually occur when the injection site does not rotate (do not stay between the shoulders) and is not administered to the muscular and nervous layers under the skin. I recommend choosing places starting one inch behind the shoulder blades, down from the back to 1 to 2 inches in front of the tail and one third to half way down to the chest and abdomen. Many people use gabapentin before injections to relieve pain. The ulcers at the injection site are cleared of surrounding hair and gently cleaned 4 or more times a day with sterile cotton swabs soaked in dilute 1: 5 household hydrogen peroxide solution. They usually do not require any more complicated treatment and will heal in about 2 weeks.
We hope that the legal form GS-441524 will be available soon. The drug, called Remdesivir, is the greatest hope today, as Remdesivir breaks down into GS immediately when given intravenously to humans, mice, primates and cats. Remdesivir has received full US FDA approval, and similar approval is likely to follow in other countries. If so, it can be prescribed by any licensed human doctor and veterinarians. However, the use of Remdesivir in the United States is still limited to a specific subset of patients with Covid-19 and only under controlled conditions and with ongoing data collection. Until all restrictions are lifted, it will not be easily accessible for human use. I have no experience treating cats with Remdesivir instead of GS-441524. However, groups in Australia and some Asian countries are starting to use Remdesivir and are reporting the same results as GS-441524. The molar basis of Remdesivir is theoretically the same as GS-441524. GS-441524 free base has a molecular weight of 291.3 g / M, while Remdesivir has 602.6 g / M. Therefore, twice as much Remdesivir (602.6 / 291.3 = 2.07) would be needed to obtain 1 mg of GS-441524. The solvent for Remdesivir differs significantly from the solvent used for GS-441524 and is intended for IV use in humans. It is not known how diluted Remdesivir will behave when administered subcutaneously for 12 weeks or more. Mild signs of hepatotoxicity and nephrotoxicity have been observed with Remdesivir in humans. GS-441524 causes mild and non-progressive renal toxicity in cats, but without apparent hepatic toxicity. It is not clear whether the renal toxicity observed in humans receiving Remdesivir is due to its active ingredient (ie GS-441524) or to chemical agents designed to increase antiviral activity. Anivive is seeking GC376 approval for cats (and humans), but it will take another two or more years. GC376 is a viral protease inhibitor and acts differently from GS-441524, which inhibits early-stage viral RNA replication. Therefore, it is unlikely to have a significant synergistic viral inhibitory effect, but will be much more important in inhibiting drug resistance when used in combination therapy (such as combination antiviral therapy for HIV / AIDS).
Sam Taylor, BVetMed (Hons), CertSAM, MANZCVS, DipECVIM-CA, FRCVS and Emi Barker BSc (Hons), BVSc (Hons), PhD, DipECVIM-CA, MRCVS summarize ideas about the manifestations and diagnosis of this disease and represent a new era of treatment .
Figure 1. “Classic” Cat with “classic” FIP with massive abdominal effusion. Image: Feline Centre, Langford Vets, University of Bristol
FIP is caused by virulent mutations in feline coronavirus (FCoV), which transform it from a mild and enteric infection to a serious systemic disease.
Like other coronaviruses, FCoV is a large enveloped RNA virus - this is important when considering immune system avoidance, environmental survival, detection, treatment and prevention. FIP has a high mortality rate and, until recently, treatments were relatively ineffective.
This article summarizes current views on the manifestations and diagnosis of this disease. It also represents a new era of FIP treatment in the context of the recent availability of legal medicines in the UK.
What causes FIP?
FCoV is an alpha-coronavirus that infects domestic cats and other cats. It is from the same genus as canine enteric coronavirus and swine gastroenteritis virus. FCoV cannot infect humans and is only distantly related to SARS-CoV-2, beta-coronavirus, and pathogen COVID-19.
FCoV, as a feline enteric coronavirus (FECV) biotype, is commonly detected in faeces - especially in cats living in multi-cat households. The infection typically spreads via the fecal-oral route when kittens or young cats are in contact with excreting cats. The chances of survival of this enveloped virus in the environment are generally poor unless the virus is trapped in feces and is sensitive to most disinfectants.
In some cats, and at some point after the initial infection - between viral replication in enterocytes and efficient replication in macrophages and monocytes - the less virulent FECV mutates into a virulent form associated with FIP - that is, the FIP virus biotype (FIPV). Certain mutations associated with this transition have been found in the spike protein gene, although none of them are yet pathognomonic for FIP.
The high frequency of genomic mutations - a hallmark of RNA viruses - can also facilitate the avoidance of the host immune response and drive tissue tropism, leading to various manifestations of the disease. Natural direct transmission of FIPV between cats is considered rare, and it is generally believed that FIPV - and subsequently FIP - results from a new mutation in the FCoV of an individually infected cat.
Figure 2. Mild jaundice and pallor in cats with FIP.
One of the many complexities of FCoV and FIP is that the infection manifests itself in many different ways depending on viral factors such as strain and dose, but also on the cat's immune response and genetic factors.
A strong cell-mediated immune (CMI) response to FCoV appears to provide protection against FIP. In contrast, cats with a predominantly antibody-mediated response with a weak CMI response typically succumb to the effusive "wet" form of the disease due to immune-mediated vasculitis, while cats with moderate CMI develop tissue granulomas typical of the non-fusive "dry" form of FIP.
It is important to keep in mind that the effusive and non-fusive forms of FIP can significantly overlap, leading to a wide range of symptoms; short episodes of the effusive form of FIP may occur rather than the predominantly non-fusive form, and conversely, effusions may form in the terminal stages of the non-fusive form of FIP. In addition, many exuded cats have tissue granulomas.
Clinical signs
Classic presentation of a young cat with protein-rich ascites (Figure 1) may offer easier diagnostics; however, other cats may be more of a diagnostic challenge. Common non-specific symptoms include lethargy, anorexia and weight loss.
Affected cats may be febrile with a moderate fever, typically less than 40 ° C, which often fluctuates and responds poorly to NSAIDs (non-steroidal anti-inflammatory drugs or non-steroidal anti-inflammatory drugs) or antimicrobials, and jaundice, if present, is usually mild (Figure 2).
Figure 3. Hyphema, uveitis and hypopyon in cats with ocular FIP.
High protein viscous effusions are formed in approximately 80% cats with FIP - most (approximately 85%) involve the abdominal cavity, while fewer cases show thoracic effusion (approximately 20%).
Pericardial effusions are occasionally observed, although rarely causing tamponade, and very rarely, scrotal effusions occur in uncastrated cats.
Pyogranulomatous lesions can occur in any tissue, and while they commonly involve the abdominal organs (e.g., mesenteric lymph nodes and kidneys), the disease may be limited to other organs such as the eyes, brain, or spinal cord.
Ocular symptoms include uveitis, ceramic clots, hypopyon, hyphaemia (Figure 3) and retinitis. Neurological symptoms include ataxia, seizures, nystagmus, hyperesthesia, and behavioral / mental changes.
Diagnosis
Although one abnormality does not in itself determine the diagnosis of FIP, nor does their absence rule out the diagnosis, the veterinarian may base the suspicion on FIP with the following findings, bearing in mind signaling, clinical picture, clinical pathology, and imaging results if no alternative diagnosis is present. , more likely explanation:
Figure 4. MRI scan of a cat with FIP showing obstructive hydrocephalus and increased contrast of the meninges.
Blood analysis - lymphopenia, non-regenerative anemia, microcytosis, neutrophilia, hyperglobulinemia, low albumin / globulin ratio (A: G; classically less than 0.4), hyperbilirubinemia, high α-1 acid glycoprotein (often markedly elevated, more than 1.5 mg / ml).
Diagnostic imaging - effusions, abdominal lesions, CNS abnormalities consistent with meningeal thickening and / or obstructive hydrocephalus (Figure 4).
Efusion analysis - non-aseptic pyogranulomatous inflammation with a relatively low cell number (total number of nuclear cells higher than 5 × 109/ l; neutrophils and macrophages) with high protein concentrations (often higher than 35 g / l) and low A: G (Figure 5).
Molecular diagnostics - positive results of FCoV RNA RT-PCR in fluids (eg effusions, aqueous humor, CSF; Note: false positive and negative results are possible in whole blood) or aspirates with a thin needle (FNA) of the affected organ (eg kidneys, liver, mesenteric lymph nodes); the higher the viral load, the more evidence of FIP. Note: RT-PCR cannot confirm the diagnosis of FIP.
High levels of FCoV antibodies indicate only previous FCoV infection and do not indicate a diagnosis of FIP
The definitive diagnosis of FIP is confirmed by positive immunohistochemical staining for coronavirus antigen in macrophages associated with pathological changes in FIP in formalin-fixed tissue samples. However, sampling for histopathology and immunohistochemical staining requires invasive procedures, which may be contraindicated in a sick cat.
Figure 5. Sweat analysis is useful in diagnosing FIP; where possible, take a fluid sample.
Alternatively, the presence of antigen-positive coronavirus cells in cytological specimens (effusion, aqueous humor, cytospin CSF preparations or FNA from any abnormal organs - such as mesenteric lymph node) showing pyogranulomatous changes is very helpful in diagnosis and allows less invasive specimen acquisition.
Some researchers have used cell pellets prepared from centrifuged effusion samples to improve the sensitivity of immunohistochemical staining (Tasker et al, 2021).
However, it is important to diagnose FIP as reliably as possible before treatment, as there are many other differential diagnoses for these clinical symptoms - including neoplasia (especially lymphoma), other infectious diseases (pyothorax, toxoplasmosis, mycobacteriosis, fungal infections)) and primary immune-mediated disease (idiopathic disease). , uveitis, lymphocyte cholangitis). On the Figure 6 is a graph indicating possible diagnostic pathways.
Minimally invasive sampling may include abdominal or thoracic effusions and FNA abnormal organs.
More detailed diagnostic flowcharts for the diagnosis of FIP are available on the website of the European Advisory Committee on Feline Diseases (www.abcdcatsvets.org/feline-infectious-peritonitis).
Figure 6. Access to FIP diagnostics
FIP treatment with antiviral drugs
In recent years, publications have focused on antiviral drugs (GS-441524, a nucleoside analog that inhibits viral RNA polymerase, and GC376, a viral protease inhibitor) with the potential to cure experimentally induced cats (Kim et al, 2016; Murphy et al, 2018) and naturally obtained (Pedersen et al, 2018; 2019; Dickinson et al, 2020) FIP.
Unfortunately, until recently (see below), legal formulations of these drugs were not commercially available, although some owners obtained and administered illegal formulations to their cats of unknown origin and at great expense.
Remdesivir, a prodrug of GS-441524, is an antiviral drug with a broad spectrum of activity against RNA viruses. It was originally developed to treat hepatitis C virus and Ebola virus in humans. Its development was then significantly accelerated due to the worldwide treatment of SARS-CoV-2.
In Australia, remdesivir has been legally available to veterinarians for several months as a "special" formulation that allows veterinarians to gain experience with this drug in the treatment of cats and kittens with FIP, where it has shown promising results. Unlike GS-441524, remdesivir has low oral bioavailability and is administered by intravenous infusion to human patients.
In the UK, remdesivir is legally available through Gilead Sciences, a patent-pending company that manufactures a medicinal product for human use. The currently available formulation is Veklury, a powder for reconstitution with water for solutions for injection to a final remdesivir concentration of 5 mg / ml. After reconstitution, it should be cooled and consumed within 24 hours.
Figure 7. Vials with reformulated remdesivir will be available to treat FIP, legally, in the UK from August 2021.
In cats, SC is usually administered unofficially, although some cats may benefit from initial IV administration. From August 2021, remdesivir will also be available from specialty drug manufacturers as a veterinary ál special ’(Figure 7) in the United Kingdom. The reformulated remdesivir will be supplied in vials containing 100 mg remdesivir, at a concentration of 10 mg / ml, allowing for smaller injection volumes, with a shelf life of at least three months when properly stored.
The experience of our colleagues from Australia (Malik, personal communication) allows us to design benefits according to the above plan. The authors emphasize the need to diagnose FIP before using this drug to ensure its proper use, while acknowledging that the diagnosis of FIP can be anticipated due to clinical or financial diagnostic limitations.
Costs, prolonged nature of the treatment cycle (recommended at least 12 weeks), potential discomfort with SC injections and risk of relapse should be discussed with cat owners before initiating therapy.
Owners may be instructed to give daily injections to their cat, but must be thoroughly trained to avoid unintentional self-administration, incorrect technique that may harm the cat, and to minimize the risk of the cat reacting to injections leading to bite or scratch injuries. This healing process requires committed owners and is an emotional as well as a significant financial commitment.
Depending on the clinical condition of the cat, supportive therapy is still needed (eg IV or SC fluids, antiemetic stimulation and appetite, analgesia, tube nutritional support, sepsis antimicrobials). Cats with uveitis may require topical treatment with corticosteroids and cats with neurological symptoms may need anti-seizure medication.
Figure 8. Bengal kitten with ocular and neurological FIP before (left) and after (right) remdesivir treatment.
Although systemic use of corticosteroids is not generally recommended concomitantly with the use of antivirals, short-term administration of corticosteroids may be considered in cats with a strong suspicion of secondary immune-mediated disease due to FIP (eg immune-mediated haemolytic anemia).
The success rate of treatment is high - 80% to 95% (Malik, personal communication; Figure 8) - and therefore we have reason to be optimistic when discussing treatment with clients, even though we are aware of the commitment and the associated costs and potential for relapse.
Increasing the success of treatment
The treatment is long and remdesivir can be painful when injected. Once opened, the medicine should be stored in the refrigerator and should be warmed to room temperature before injection. Needle size can affect discomfort; for some patients, a faster injection of a larger diameter "green" needle (21G) may be more advantageous, while a smaller diameter orange "orange" (25G) needle may be more advantageous. A new needle should be used for each injection.
Some cats will need to go to the clinic every day for an injection. Gabapentin or trazodone (both 50 mg to 100 mg orally per cat), given two hours before the deadline to reduce anxiety and pain, may benefit some cats. Other cats may need a dose of buprenorphine (0.02 mg / kg to 0.03 mg / kg transmucosally or IM in a clinic before treatment).
To reduce discomfort, the injection site can be trimmed and EMLA topical anesthetic cream applied 45 to 60 minutes before injection. Injection tolerance appears to vary between cats.
Remdesivir in the treatment of FIP
Dosage
FIP s exudates (ie ascites and / or pleural effusion), but without any ocular or neurological impairment: 7 mg / kg until 8mg / kg once a day.
FIP s ocular symptoms (that is, uveitis or other eye disorders, but without neurological impairment): 10 mg / kg once a day.
FIP s neurological symptoms: 12 mg / kg until 15mg / kg once a day.
Method of administration
Most cases: SC injection into the loose skin of the interscapular area.
Very severe cases: 10 mg / kg may initially be given by intravenous infusion (ie diluted in 10 ml saline and given slowly over 10 to 20 minutes) to achieve a rapid antiviral effect; This can be done after three to four days of SC injection as soon as the cat starts eating and its health improves. Note: After intravenous administration, some cats may experience depression for several hours.
Duration of treatment
Treatment of at least 84 days (ie 12 weeks) should be considered. This time is based on a clinical study with GS-441524 and the unofficial use of remdesivir to minimize the likelihood of FIP relapse.
After 84 days, treatment should only be discontinued if the patient is clinically OK and abnormal laboratory parameters have returned to normal.
If the response to treatment is only partial or unsatisfactory, a prolongation of treatment may be necessary.
Monitoring
In the first days, closely monitor for clinical signs: - Improvement should be rapid, within a few days, with weight gain and improvement in clinical symptoms. - Consider verifying the diagnosis if no improvement is seen (with regard to the following symptoms): • Efusion (especially pleural) may worsen for one to two days at the start of treatment and may require therapeutic thoracocentesis or abdominocentesis. This appears to occur most frequently after IV treatment. Consider ultrasound monitoring once or twice daily. • Neurological symptoms may initially appear or worsen in the first days of treatment. This may include the development of seizures that may require medical attention (eg levetiracetam 20 mg / kg to 30 mg / kg every eight hours).
The weight should be checked regularly and the doses adjusted accordingly.
Monitor PCV, total proteins (albumin and globulin), bilirubin and other abnormal parameters until they return to normal. The frequency of monitoring varies between veterinarians; a monthly assessment of biochemistry and hematology is usually performed, but should be adapted to the client's finances and the cat's response and behavior.
Serum globulins may increase initially, but any hyperglobulinemia usually resolves by week 12.
Remdesivir is reported to cause reno / hepatotoxicity in humans, but these have only been observed at higher doses by our Australian colleagues, who resigned when the dose was reduced. * Higher doses may be required depending on the response. Using lower doses to reduce costs may increase the likelihood of treatment failure. Please note that these dosing recommendations may change depending on the growing amount of data and clinical experience of veterinarians using this medicine. It is recommended to consult an expert in cats or internal medicine to discuss the individual case and the appropriate dosage.
Further treatment
The researchers are looking at the beneficial effects of immunostimulants and / or other antiviral medicines, such as interferons or mefloquine, once remdesivir treatment is stopped or if the injections are considered too painful. Most studies published to date have focused on the use of antiviral drugs alone.
Thanks
The authors would like to thank their Australian colleagues David Hughes, Rebecca Brady and Richard Malik for sharing their experiences with remedivirus treatment in cats with FIP. Thanks also to Séverine Tasker and Professor Gunn-Moore for comments on the article.
Do you need advice on FIP treatment?
Stephanie Sorrell and Danièlle Gunn-Moore of the University of Edinburgh will recruit cases to monitor the UK's response to the remdesivir, with more information coming soon.
If advice is needed in the meantime on the diagnosis and treatment of a suspected FIP case, send an e-mail to fipadvice@gmail.com
References
Dickinson PJ, Bannasch M, Thomasy SM, Murthy VD, Vernau KM, Liepnieks M, Montgomery E, Knickelbein KE, Murphy B and Pedersen NC (2020). Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis, Journal of Veterinary Internal Medicine34(4): 1,587-1,593.
Kim Y, Liu H, Galasiti Kankanamalage AC, Sahani Weerasekara S, Hua DH, WC Groutas, Chang K and Pedersen NC (2016). Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor, PLOS Pathogens12(3): e1005531.
Murphy BG, Perron M, Murakami E, Bauer K, Park Y, Eckstrand C, Liepnieks M and Pedersen NC (2018). The nucleoside analog GS-441524 strongly inhibits feline infectious peritonitis (FIP) virus in tissue culture and experimental cat infection studies, Veterinary Microbiology219: 226-233.
Pedersen NC, Kim Y, Liu H, Galasiti Kankanamalage AC, Eckstrand C, Groutas WC, Bannasch M, Meadows JM and Chang KO (2018). Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis, Journal of Feline Medicine and Surgery20(4): 378-392.
Pedersen NC, Perron M, Bannasch M, Montgomery E, Murakami E, Liepnieks M and Liu H (2019). Efficacy, and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis, Journal of Feline Medicine and Surgery21(4): 271-281.
Authors: Linda Brunotte, Shuyu Zheng, Angeles Mecate-Zambrano, Jing Tang, Stephan Ludwig, Ursula Rescher, and Sebastian Schloer
Abstract
The ongoing SARS-CoV-2 pandemic requires effective and safe antiviral treatment strategies. Drug repurposing is a fast and inexpensive approach to developing new treatment options. The direct antiviral agent remdesivir was found to have antiviral activity against SARS-CoV-2. While remdesivir has only a very short half-life and bioactivation, which depends on prodrug activating enzymes, its plasma metabolite GS-441524 can be activated by various kinases, including adenosine kinase (ADK), which is moderately expressed in all tissues. The pharmacokinetics of GS-441524 suggest that it is a suitable antiviral drug that can be administered to patients with COVID-19. In this work, we analyzed the antiviral properties of combination therapy with the metabolite remdesivir GS-441524 and the antidepressant fluoxetine in a polarized Calu-3 cell culture model against SARS-CoV-2. Combination therapy with GS-441524 and fluoxetine was well tolerated and showed synergistic antiviral effects against the three circulating SARS-CoV-2 variants in vitro in commonly used drug interaction reference models. Thus, combination treatment with GS-441524 virus-targeted and host-targeted fluoxetine could offer a suitable therapeutic option for the treatment of SARS-CoV-2 infections.
Translator's note: Fluoxetine is produced under various trade names, of which Prozac is probably the best known.