

Katarina Hazuchova, Susanne Held, Reto Neiger
Original article: Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions: 18.7.2016; Translation 28.3.2021
Abstract
Goals
The aim of this study was to evaluate acute phase protein (APP) measurements as a diagnostic tool to distinguish between feline infectious peritonitis (FIP) and other diseases in cats with body cavity effusions.
Methods
Cats with pleural, abdominal or pericardial effusion have been included prospectively. Cats were classified as FIP positive or negative based on immunohistochemistry (if available) or a sophisticated statistical method using machine learning methodologies using concepts from game theory. FIP-free cats were further divided into three subgroups: heart disease, neoplasia and other diseases. Serum amyloid A (SAA), haptoglobin (Hp) and α1-acid glycoprotein (AGP) were measured in serum and exudate using previously validated tests in cats.
The results
Serum and effusion samples from 88 and 88, respectively, were available for APP measurement. 67 cats. Serum and effusion APP concentrations were significantly different in cats with and without FIP (P <0.001 for all three APPs). The best APP to distinguish between cats without FIP was AGP in effusion; the cut-off value of 1550 µg / ml had a sensitivity and specificity of 93% for the diagnosis of FIP.
Conclusions and significance
AGP has been found, especially when measured in effusion, to be useful in distinguishing between FIP and other diseases, while SAA and Hp are not. The concentration of all three APPs in some diseases (e.g. septic processes, disseminated neoplasia) was as high as in cats with FIP; so none of them can be recommended as a single diagnostic test for FIP.
Introduction
Feline infectious peritonitis (FIP) is a fatal infectious disease that can occur in two clinically distinct forms, the more common effluent (wet) form and the granulomatous (dry) form.1-3 Abdominal distension and dyspnoea are common in cats with effusive FIP. Ascites or pleural effusion caused by FIP is important to distinguish from other potential causes such as heart disease, neoplasia or septic effusion.4,5 Although several diagnostic tests have been developed for the diagnosis of FIP, differentiation between FIP and diseases with similar clinical manifestations remains a challenge. Although recent advances in the development of antiviral drugs may change the outcome of the disease in the future, 6 there is currently no widely available effective treatment for FIP (translator's note - as we know, treatment already exists - the article is from 2016). It is essential to make a correct diagnosis, as the consequences are currently fatal. In most cases, a combination of several diagnostic tests is necessary.3
Because FIP is an inflammatory condition, an increase in acute phase protein (APP) concentrations can be expected. APPs are produced by hepatocytes as part of an acute phase response, which is an early and non-specific but very complex response of the body to various injuries (infection, trauma, necrosis, malignant growth, etc.). 7-9 Depending on the extent of their response to triggers, APPs can be classified as major (10- to 100-fold increase), mean (two- to ten-fold increase), and minor (10- to 100-fold increase). <dvojnásobné zvýšenie). U mačky sú hlavnými APP sérový amyloid A (SAA) a α1-kyslý glykoproteín (AGP); haptoglobín (Hp) je priemerný APP.10
Several studies have examined the diagnostic potential of APP in the diagnosis of FIP, as well as the possible role of APP in the pathogenesis of FIP. 11–17 These researches had certain disadvantages that limited the implementation of the results in practice. First, APP in cats with FIP was compared with APP in healthy cats or cats exposed to feline coronavirus (FCoV) (based on FCoV positive titer) instead of comparison with cats potentially suffering from FIP, based on similar clinical manifestations.11,13 Second, it was not clear whether effusion or serum was used to measure APP.12 In addition, the sample size was too small to draw meaningful conclusions, as only four cats without FIP and eight cats with FIP were included in one study.
The aim of this study was to evaluate the ability of APP (measured in serum and effusion) to distinguish FIP from other diseases.
Materials and methods
The study prospectively included cats with pleural, abdominal, or pericardial effusions or a combination thereof, which were examined at a small animal clinic at Justus-Liebig University in Giessen, Germany, and Tierklinik Hofheim, Germany, for a period of two years. Abdomino, thora- or pericardiocentesis were performed as routine diagnostic procedures to examine the nature of the disease process in each cat. Cats from which less than 5 ml of effusion could be obtained were excluded from this study.
Routine serum hematology and biochemistry, tests for antibodies to feline immunodeficiency virus (FIV) and feline leukemia virus (FeLV) antigen (SNAP FIV / FeLV Combo Test; IDEXX Laboratories) as well as standard laboratory analysis (total content) were performed on all cats. protein, albumin and total number of nucleated cells) and cytological examination of the effusion. Residual serum and effluent samples were stored for up to 24 months at -80 ° C until APP was analyzed.
In connection with FIP, several diagnostic tests have been performed in other studies, namely the Rivalt effusion test, the anti-FCoV antibody test in serum and effusion, immunofluorescence staining of the FCoV antigen in effusion macrophages, PCR in EDTA blood and effusion. 18 The rival's test was performed in a central laboratory at a small animal clinic, as mentioned above.19 Direct and indirect detection of FCoV was performed at the Justus-Liebig University Institute of Veterinary Virology in Giessen, with the exception of immunofluorescence staining of FCoV antigen in effusion macrophages, which was performed in an external laboratory (Landesbetrieb Hessisches Landeslabor, Giessen). Anti-FCoV antibody titers were determined by indirect immunofluorescence assay using a methodology similar to the previous study.20 Embedded PCR with reverse transcriptase from EDTA blood and effusion was performed by the method of Herrewegh et al. 21 Immunofluorescence staining of FCoV antigen in effusion macrophages was performed by a method identical to that used by Parodi et al. 22 Additional diagnostic procedures (thoracic and / or abdominal radiography, abdominal ultrasonography, CT, echocardiography, cytology, histopathology, chest or abdomen surgical examination) were performed depending on the medical condition. Cats that died or were killed during hospitalization were subjected to a post-mortem inspection at the Justus-Liebig Institute for Veterinary Pathology, Giessen University, subject to the owner's consent. Pathohistological examination included immunohistochemistry as the gold standard for the diagnosis of FIP according to the method described by Kipar et al. 23
The final diagnosis (FIP vs. non-FIP) in the previous study was made based on the results of immunohistochemistry, if possible.18 The remaining cats, for which no immunohistochemistry was available, either because the cats were discharged from the clinic or the owners refused postmortem examination, were classified as FIP-positive or FIP-negative using a sophisticated statistical method.24 This method combines machine learning methodology with partial supervision using concepts from cooperative game theory using the results of several diagnostic tests in individuals whose actual state of health is unknown.24 The method takes into account the accuracy of diagnostics and the clinical significance of individual tests and their combinations for the determination of the final diagnosis. Briefly, 29/100 cats included in the previous study underwent post mortem examination (including immunohistochemistry).18 and 11/29 cats were diagnosed with FIP. Results of several diagnostic tests (Rivalta effusion test, anti-FCoV antibody test in serum and effusion, immunofluorescent staining of FCoV antigen in effluent macrophages, PCR in EDTA blood and effusion) from 16/29 cats for which FIP / non-FIP status was known on the basis of immunohistochemistry, were used to teach the device. The remaining 13/29 cats were used as test samples. Using this statistical method, the FIP / non-FIP status of the remaining 71 cats in the previous study was then evaluated.
Cats without FIP were further divided according to the results of all diagnostic tests into three subgroups: (1) heart disease - cats in which echocardiography diagnosed effusion cardiomyopathy; (2) neoplasia - cats in which it has been possible to diagnose a tumor causing effusion on the basis of cytological and / or histological examination; and (3) others - cats with effusion caused by a disease other than FIP, heart disease or tumor.
The cats included in this study represent a subset of the population from previous research.18 The classification of cats into the FIP / non-FIP category, as well as the further classification of cats without FIP into three subgroups (heart disease, neoplasia, etc.), was performed in the same manner as in this study.
Measurement of acute phase proteins
Serum and effluent samples were thawed at room temperature before measuring APP. The presence of hemolysis was assessed visually.
Haptoglobin and SAA were measured with an ABX Pentra 400 automated analyzer (Axon Lab) using reagents from the Phase Range Haptoglobin kit (second generation) (Tridelta Development) and the LZ Test 'Eiken' SAA (Eiken Chemical). Both tests were used to measure APP in cats. 11,25,26 AGP was measured by the manual method using reagents from the SRID Assay Kit (Phidel Feline α1 Acid Glycoprotein) (Tridelta Development). This test has also been validated and used in cats. 13,14
Statistical analysis
The data were tested for normality using the D'Agostino and Pearson summary normality test and found not to be normally distributed. Numeric values are therefore given as median and range. APPs in cats with and without FIP were compared using the Mann-Whitney U-test, while the four groups (depending on the final diagnosis) were compared using the Kruskal-Wallis test, followed by Dunn's comparison. Receiver operating characteristic curves (ROC) and area under the curve (AUC) were calculated for each parameter tested. Statistical analysis was performed using commercial software (GraphPad Prism version 6). Statistical significance was defined as P ⩽0.05.
The results
Serum samples were available for APP measurement from 88 cats. In 67/88 cats, APP was also measured in effusion. The median age of the 88 cats was 8.3 years (range 0.3-17.9 years); the age of the four cats was unknown. Thirty (34%) cats were females (four intact, 26 sterilized) and 57 (65%) males (seven intact, 50 neutered); in one (1%) cat, gender was not recorded. The most common breed was the domestic shorthair (63 cats [72%]); Another 11 breeds were recorded. Thirty-seven (42%) cats had ascites, 44 (50%) cats had pleural effusion, five (6%) cats had ascites and pleural effusion, and two (2%) cats had pericardial effusion. Of the 88 cats, 20 (23%) cats had FIP (nine cats confirmed this by immunohistochemistry; the remaining 11 cats were found statistically) and 68 (77%) cats had other diseases (16 cats were diagnosed by histopathology). Of these, 22 (25%) cats had heart disease, 24 (27%) had tumor and 22 (25%) cats had other diseases. In the second group, the diagnosis was made in all but two cats. Cats were diagnosed with one of the following diseases: septic peritonitis or pyothorax (n = 10), sepsis (with chest effusion classified as transudate based on cell number and total protein; n = 1), idiopathic chylothorax (n = 3), kidney disease ( n = 2), hepatic amyloidosis (n = 1), cholangiohepatitis (n = 1), permethrin intoxication (n = 1) and trauma (n = 1).
Two cats were positive for FIV, two for FeLV and one was positive for both FIV and FeLV. The underlying diseases responsible for effusion in these cats were FIP, septic peritonitis, carcinoma, lymphoma and trauma.
Three serum samples and 12 effusion samples were markedly hemolytic.
Serum and effusion concentrations of the three APPs were significantly different in cats with and without FIP (P <0.001 for all three APPs) (Table 1).
| FIP | Non-FIP | P value | ||
|---|---|---|---|---|
| Serum | Hp (mg / ml) | 2.0 (2.0-9.0) | 1.8 (0-2.0) | <0.001 |
| AGP (μg / ml) | 2900 (960-5040) | 690 (120-4500) | <0.001 | |
| SAA (μg / ml) | 98.5(1.3-163.4) | 7.6(0.1-163.8) | <0.001 | |
| Effusion | Hp (mg / ml) | 2.2(0.1-9.3) | 0.8(0.1-2.5) | <0.001 |
| AGP (μg / ml) | 2570(1300-5760) | 480 (190-3800) | <0.001 | |
| SAA (μg / ml) | 80.4(0.1-207.4) | 0.1 (0.1-182.7) | <0.001 |
There was a significant difference in serum and effusive concentrations of all three APP concentrations between cats with FIP, heart disease, neoplasias, and others (Figures 1a – ca 2a, b), with the sole exception of serum SAA, which did not differ between cats with FIP and other diseases (Figure 2c).


The ROC curves for the three APPs in the diagnosis of FIP are shown for the serum in Figure 3 and for the effusion in Figure 4.

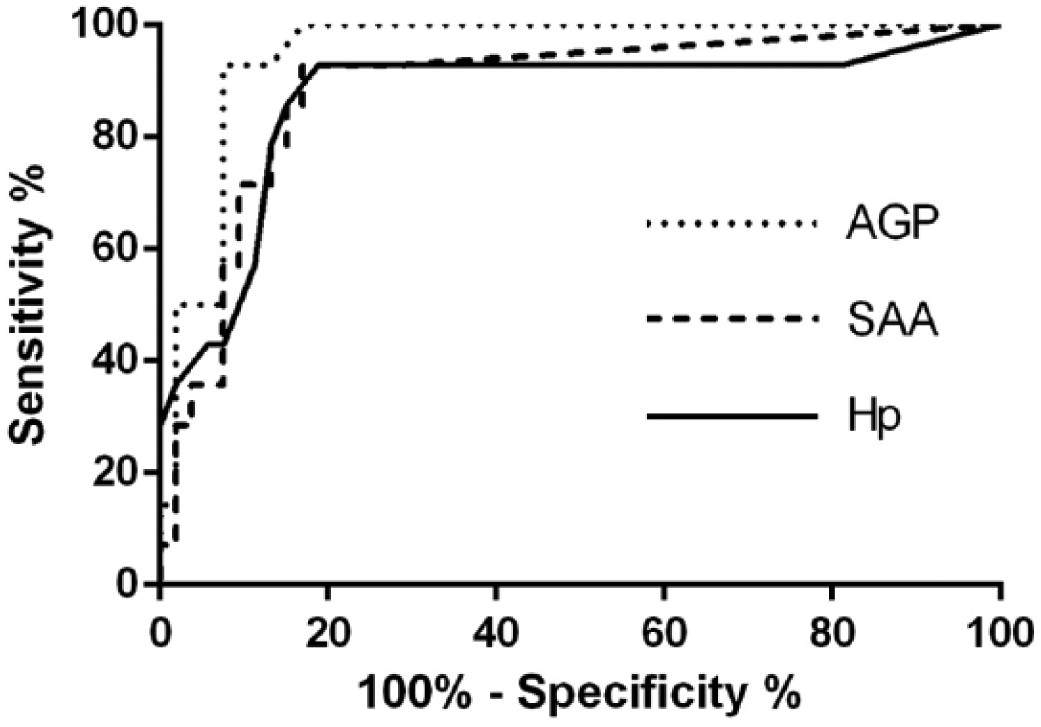
Table 2 shows the AUC for each APP, including the best cut-off values based on the ratio of the best probability to its sensitivity and specificity.
| AUC | Cut-off | Sensitivity (%) | Specificity (%) | ||
|---|---|---|---|---|---|
| Serum | Hp | 0.777 | 2.0 mg / ml | 55 | 82 |
| AGP | 0.899 | 2260 μg / ml | 85 | 90 | |
| SAA | 0.800 | 97.3 μg / ml | 55 | 87 | |
| Effusion | Hp | 0.870 | 2.1 mg / ml | 79 | 87 |
| AGP | 0.950 | 1550 μg / ml | 93 | 93 | |
| SAA | 0.885 | 43.6 μg / ml | 71 | 91 |
AGP in effusion has been shown to be the best marker for distinguishing FIP from other diseases; the cut-off value of 1550 μg / ml had a sensitivity and specificity of 93% for the diagnosis of FIP.
Discussion
This is the first study to evaluate all three important APPs in cats, measured in serum and effusion, as a diagnostic tool to distinguish FIP from other diseases. The best APP to distinguish cats with or without FIP was AGP in effusion. The AUC of the ROC curve for this analyte was 0.95; the cut-off value of 1550 μg / ml had a sensitivity and specificity of 93% for the diagnosis of FIP. The cut-off values for the tested parameters were chosen preferentially to obtain high specificity, as a false positive result could be potentially fatal for the cat. In the present study, only four cats with non-FIP diseases had effusion AGP concentrations higher than 1550 μg / ml and would therefore be falsely diagnosed with FIP. Of these cats, three had septic effusion and one had metastatic pancreatic carcinoma, endocarditis, and purulent bronchopneumonia. This cat had ascites, and although no tumor cells were found on cytology, the cause was most likely metastatic pancreatic cancer and the cat was classified as a "tumor group." However, this cat also tested positive for FIV and FeLV, which may have affected APP levels. As FIV or FeLV contributed to APP concentrations in the remaining four cats with FIV and / or FeLV, it is not possible to determine using current methods.
In all APPs tested in serum and effusion, some cats with septic processes and several cats with disseminated neoplasms had APP levels as high as cats with FIP. However, cats with heart disease had low APP, with the sole exception of one cat with endocarditis with an AGP concentration at an effusion of 1500 μg / ml. This cat also showed signs of bronchopneumonia at post-mortem examination, which probably contributed to the high concentration of AGP. However, this cat was classified as a "heart disease" because AGP was measured in ascites, which was considered a secondary consequence of heart failure based on post-mortem and cytological findings (modified transudate). Interestingly, in all APPs when measuring APP in effusion, there was less overlap between cats with FIP and cats with septic or neoplasia. The cause of this finding is currently unknown.
Based on these findings, a proposed diagnostic algorithm could be useful in clinical practice. In cats with body effusions, AGP in effusions should be determined. If AGP levels are high, FIP or septic or disseminated neoplastic disease should be considered. Septic effusion can be easily identified by the results of hematology and cytological examination of the effusion. If there is no evidence of a septic process, additional FIP diagnostic tests should be performed. The main disadvantage of this diagnostic algorithm is the poor availability of AGP testing compared to other methods, including PCR. However, this could be improved in the future by introducing tests that can be used with automated analyzers.27
Several studies have found elevated APP levels in cats with FIP; 11–14, however, high levels of APP have also been reported in a variety of other inflammatory and non-inflammatory conditions, such as neoplasia. 25,26,28–30 Two studies in cats with FIP evaluated only AGP, 13,14 and one study evaluated both AGP and Hp.12 All three APPs have also been the subject of other research; however, the results were only compared with those in healthy cats.11 In one study, the ROC curve for serum AGP showed an AUC of 0.850,13, which is similar to the value found in the current research (0.899). However, clinically healthy cats were used to calculate the ROC in this study, which prevented direct comparison of results.13 For sensitivity AGP, excellent sensitivity and specificity have been reported for the diagnosis of FIP, each with 100% specificity using a cut-off value of 1.5 mg / ml (ie 1500 /g / ml).14 However, only eight cats with FIP and four cats with other diseases were included and these results should be interpreted with caution. Using the same cut-off value, AGP had a sensitivity of 85% and a specificity of 100% in another study.12 This excellent specificity can be attributed to the fact that no cats with septic effusion were included.12 Septic cats, according to this study, have AGP values as high as cats with FIP, which reduces the specificity of this parameter.
There are several limitations in this study. First, immunohistochemistry, the gold standard method for diagnosing FIP, could only be performed in 11 cats for confirmation and in 18 cats for FIP exclusion (cats suffering from diseases other than FIP) because post-mortem examination was performed only in this subgroup of cats.18 However, in the latest comprehensive review of FIP diagnosis, histological examination and immunohistochemistry were not considered necessary requirements for FIP diagnosis.31 Instead, the typical characteristics, anamnesis, and clinical signs of FIP have proven to be important diagnostic tools. However, the limitations of every laboratory method, including immunohistochemistry, have also emerged.31 Other authors based the diagnosis of FIP on the findings of cytological examination of the effusion in combination with other laboratory parameters and a typical history for cases where histology was not available.32,33 To overcome the problem of the absence of post-mortem examinations, a highly reliable and sophisticated statistical method combining the results of several tests was used to classify FIP positive or FIP negative cats.24
The assays used to measure APP were not specifically designed to measure these analytes in effusion. However, according to the manufacturer's instructions, the AGP tests in this study can be used to determine the concentration of AGP in feline serum or other samples. A similar test was previously used to measure AGP in effusion.12 Long-term storage may have affected APP concentrations in our samples, as some were stored for up to 2 years at -80 ° C prior to analysis.
It is known that some laboratory methods are affected by the presence of hemolysis, lipemia and bilirubinemia in the analyzed samples. We still do not have much information about the effect of these substances on the measurement of APP in dogs and cats.10 To our knowledge, no specific measures have been published for the immunoturbidimetric assay used to measure the concentration of SAA or single radial immunodiffusion used to measure the concentration of AGP in cats in this study. When measuring the Hp concentration, haemolysis could be of concern, as free hemoglobin could bind to haptoglobin in the sample, which in turn could lead to falsely reduced Hp concentrations. 34 Because hemolytic samples were not excluded from the analysis, their use could affect the results and could be responsible for the limited usefulness of Hp in the diagnosis of FIP.
In conclusion, it is important to emphasize that the findings of this study are only applicable to cats with effusions in body cavities, which may suffer from the effusive (wet) form of FIP. Further studies are needed to evaluate APP in cats with granulomatous (dry) FIP.
Conclusions
Although AGP has been found to be a useful diagnostic tool for distinguishing between FIP and other diseases causing effusion, the contribution of SAA and Hp has not been sufficient in this regard. Measurement of AGP in effusion provided the highest diagnostic benefit among APPs tested in both serum and effusion. However, because some AGP overlap has been found in cats with FIP and septic disease or disseminated neoplasia, AGP cannot be used as the sole test for FIP.
Thanks
We would like to thank Sabina Zielinska for technical support and all colleagues from the Clinic of Small Animals and Dr. Christiane Stengel from Tierklinik Hofheim, Germany, for sampling.
Conflict of interests
The authors did not indicate any potential conflict of interest in connection with the research, authorship or publication of this article.
Financing
The authors have not received any financial support for the research, authorship and / or publication of this article.
Part of this study was presented as an oral abstract presentation at the 22nd Annual ECVIM-CA Congress in 2012 in Maastricht, the Netherlands.
Received: June 16, 2016
References
| 1. | Wolfe, RG, Griesemer, LA. Feline infectious peritonitis. Pathol Vet 1966; 3: 255–270. Google Scholar | SAGE Journals |
| 2. | Montali, RJ, Strandberg, JD. Extraperitoneal lesions in feline infectious peritonitis. Vet Pathol 1972; 9: 109–121. Google Scholar | SAGE Journals | ISI |
| 3. | Pedersen, NC. A review of feline infectious peritonitis virus infection: 1963–2008. J Feline Med Surg 2009; 11: 225–258. Google Scholar | SAGE Journals | ISI |
| 4. | Tasker, S, Gunn-Moore, D. Differential diagnosis of ascites in cats. In Pract 2000; 22: 472–479. Google Scholar | Crossref |
| 5. | Beatty, J, Barrs, V. Pleural effusion in the cat: a practical approach to determining aetiology. J Feline Med Surg 2010; 12: 693–707. Google Scholar | SAGE Journals | ISI |
| 6. | Kim, Y, Liu, H, Galasiti Kankanamalage, AC. Reversal of the progression of fatal coronavirus infection in cats by a broad-spectrum coronavirus protease inhibitor. PLoS Pathog 2016; 12: e1005531. Google Scholar | Crossref | Medline | ISI |
| 7. | Kushner, I. The phenomenon of the acute phase response. Ann NY Acad Sci 1982; 389: 39–48. Google Scholar | Crossref | Medline | ISI |
| 8. | Baumann, H, Gauldie, J. The acute phase response. Immunol Today 1994; 15: 74–80. Google Scholar | Crossref | Medline |
| 9. | Koj, A. Initiation of acute phase response and synthesis of cytokines. Biochim Biophys Acta 1996; 1317: 84–94. Google Scholar | Crossref | Medline | ISI |
| 10. | Cerón, JJ, Eckersall, PD, Martínez-Subiela, S. Acute phase proteins in dogs and cats: current knowledge and future perspectives. Vet Clin Path 2005; 34: 85–99. Google Scholar | Crossref | Medline | ISI |
| 11. | Giordano, A, Spagnolo, V, Colombo, A. Changes in some acute phase protein and immunoglobulin concentrations in cats affected by feline infectious peritonitis or exposed to feline coronavirus infection. Vet J 2004; 167: 38–44. Google Scholar | Crossref | Medline | ISI |
| 12. | Duthie, S, Eckersall, PD, Addie, DD. Value of α1-acid glycoprotein in the diagnosis of feline infectious peritonitis. Vet Rec 1997; 141: 299–303. Google Scholar | Crossref | Medline | ISI |
| 13. | Paltrinieri, S, Alessia, G, Vito, T. Critical assessment of the diagnostic value of feline α1-acid glycoprotein for feline infectious peritonitis using the likelihood ratios approach. J Vet Diagn Invest 2007; 19: 266–272. Google Scholar | SAGE Journals | ISI |
| 14. | Giori, L, Giordano, A, Giudice, C. Performances of different diagnostic tests for feline infectious peritonitis in challenging clinical cases. J Small Anim Pract 2011; 52: 152–157. Google Scholar | Crossref | Medline | ISI |
| 15. | Paltrinieri, S, Metzger, C, Battilani, M. Serum α1-acid glycoprotein (AGP) concentration in non-symptomatic cats with feline coronavirus (FCoV) infection. J Feline Med Surg 2007; 9: 271–277. Google Scholar | SAGE Journals | ISI |
| 16. | Paltrinieri, S, Gelain, ME, Ceciliani, F. Association between faecal shedding of feline coronavirus and serum α1-acid glycoprotein sialylation. J Feline Med Surg 2008; 10: 514–518. Google Scholar | SAGE Journals | ISI |
| 17. | Ceciliani, F, Grossi, C, Giordano, A. Decreased sialylation of the acute phase protein α1-acid glycoprotein in feline infectious peritonitis (FIP). Vet Immunol Immunopathol 2004; 99: 229–236. Google Scholar | Crossref | Medline | ISI |
| 18. | Held, S. Accuracy diagnostic tests for Feline Infectious Peritonitis (FIP) in cats with a body height test. Dissertation, Justus-Liebig University Giessen, 2013. Google Scholar |
| 19. | Hirschberger, J. Körperhöhlenergüsse. In: Kraft, W, Dürr, UM (eds). Clinical laboratory diagnostics in animal health. 6th ed. Stuttgart: Schattauer, 2005, p 243. Google Scholar |
| 20. | Pratelli, A. Comparison of serologic techniques for the detection of antibodies against feline coronaviruses. J Vet Diagn Invest 2008; 20: 45–50. Google Scholar | SAGE Journals | ISI |
| 21. | Herrewegh, AAPM, DeGroot, RJ, Cepica, A. Detection of feline coronavirus RNA in feces, tissues, and body fluids of naturally infected cats by reverse transcriptase PCR. J Clin Microbiol 1995; 33: 684–689. Google Scholar | Crossref | Medline | ISI |
| 22. | Parodi, MC, Cammarata, G, Paltrinieri, S. Using direct immunofluorescence to detect coronaviruses in peritoneal and pleural effusions. J Small Anim Pract 1993; 34: 609–613. Google Scholar | Crossref | ISI |
| 23. | Kipar, A, Bellmann, S, Gunn-Moore, DA. Histopathological alterations of lymphatic tissues in cats without feline infectious peritonitis after long-term exposure to FIP virus. Vet Microbiol 1999; 69: 131–137. Google Scholar | Crossref | Medline | ISI |
| 24. | Pfannschmidt, K, Hüllermeier, E, Held, S. Evaluating tests in medical diagnosis: combining machine learning with game-theoretical concepts. Proceedings IPMU-2016 International Conference on Information Processing and Management of Uncertainty in Knowledge Based Systems; 2016 Jun 20–24; Eindhoven, The Netherlands. Springer, 2016, pp 450–461. DOI: 10.1007 / 978-3-319-40596-4 38. Google Scholar | Crossref |
| 25. | Hansen, AE, Schaap, MK, Kjelgaard-Hansen, M. Evaluation of a commercially available human serum amyloid A (SAA) turbidimetric immunoassay for determination of feline SAA concentration. Vet Res Commun 2006; 30: 863–872. Google Scholar | Crossref | Medline | ISI |
| 26. | Tamamoto, T, Ohno, K, Ohmi, A. Verification of measurement of the feline serum amyloid A (SAA) concentration by human SAA turbidimetric immunoassay and its clinical application. J Vet Med Sci 2008; 70: 1247–1252. Google Scholar | Crossref | Medline |
| 27. | Bence, LM, Addie, DD, Eckersall, PD. An immunoturbidimetric assay for rapid quantitative measurement of feline alpha-1-acid glycoprotein in serum and peritoneal fluid. Vet Clin Pathol 2005; 34: 335–340. Google Scholar | Crossref | Medline | ISI |
| 28. | Kajikawa, T, Furuta, A, Onishi, T. Changes in concentrations of serum amyloid A protein, α1-acid glycoprotein, haptoglobin, and C-reactive protein in feline sera due to induced inflammation and surgery. Vet Immunol Immunopathol 1999; 68: 91–98. Google Scholar | Crossref | Medline | ISI |
| 29. | Sasaki, K, Ma, Z, Khatlani, TS. Evaluation of feline serum amyloid A (SAA) as an inflammatory marker. J Vet Med Sci 2003; 65: 545–548. Google Scholar | Crossref | Medline | ISI |
| 30. | Selting, KA, Ogilvie, GK, Lana, SE. Serum alpha 1-acid glycoprotein concentrations in healthy and tumor bearing cats. J Vet Intern Med 2000; 14: 503–506. Google Scholar | Medline | ISI |
| 31. | Pedersen, NC. An update on feline infectious peritonitis: diagnostics and therapeutics. Vet J 2014; 201: 133–141. Google Scholar | Crossref | Medline | ISI |
| 32. | Gamble, DA, Lobbiani, A, Gramegna, M. Development of a nested PCR assay for detection of feline infectious peritonitis virus in clinical specimens. J Clin Microbiol 1997; 35: 673–675. Google Scholar | Crossref | Medline | ISI |
| 33. | Ishida, T, Shibanai, A, Tanaka, S. Use of recombinant feline interferon and glucocorticoid in the treatment of feline infectious peritonitis. J Feline Med Surg 2004; 6: 107–109. Google Scholar | SAGE Journals | ISI |
| 34. | Eckersall, PD, Duthie, S, Safi, S. An automated biochemical assay for haptoglobin: prevention of interference from albumin. Comp Haematol Int 1999; 9: 117–124. Google Scholar | Crossref |